

Morphology and Molecular Features of Rare Colorectal Carcinoma Histotypes
- PMID: 31340478
- PMCID: PMC6678907
- DOI: 10.3390/cancers11071036
Morphology and Molecular Features of Rare Colorectal Carcinoma Histotypes
Abstract
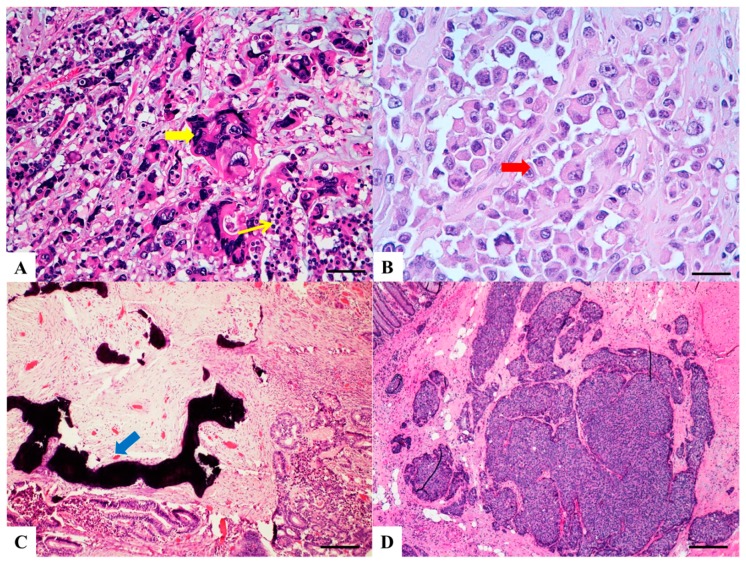
Several histopathological variants of colorectal carcinoma can be distinguished, some associated with specific molecular profiles. However, in routine practice, ninety/ninety-five percent of all large bowel tumors are diagnosed as conventional adenocarcinoma, even though they are a heterogeneous group including rare histotypes, which are often under-recognized. Indeed, colorectal cancer exhibits differences in incidence, location of tumor, pathogenesis, molecular pathways and outcome depending on histotype. The aim is therefore to review the morphological and molecular features of these rare variants of intestinal carcinomas which may hold the key to differences in prognosis and treatment.
Keywords: adenocarcinoma with osseous metaplasia; clear cell carcinoma; colorectal cancer histotypes; cribriform/comedo-type carcinoma; hepatoid carcinoma; lymphoepitelioma-like carcinoma; medullary carcinoma; micropapillary carcinoma; rhabdoid carcinoma; signet ring cell carcinoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Remo A., Pancione M., Zanella C., Vendraminelli R. Molecular pathology of colorectal carcinoma. A systematic review centred on the new role of the pathologist. Pathologica. 2012;104:432–441. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
