

Diagnosis of elevated intracranial pressure in critically ill adults: systematic review and meta-analysis
- PMID: 31340932
- PMCID: PMC6651068
- DOI: 10.1136/bmj.l4225
Diagnosis of elevated intracranial pressure in critically ill adults: systematic review and meta-analysis
Abstract
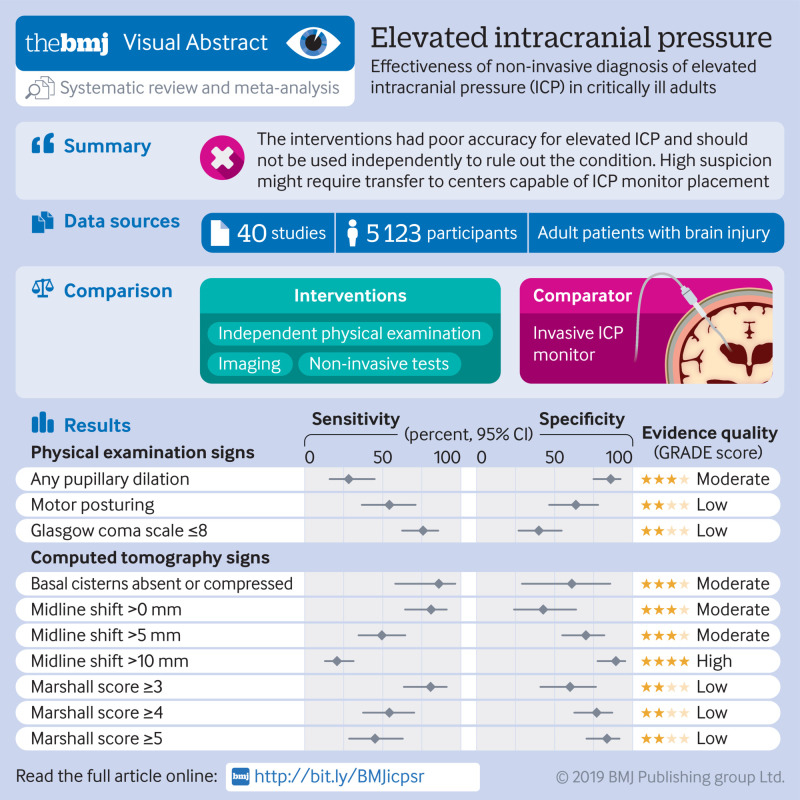
Objectives: To summarise and compare the accuracy of physical examination, computed tomography (CT), sonography of the optic nerve sheath diameter (ONSD), and transcranial Doppler pulsatility index (TCD-PI) for the diagnosis of elevated intracranial pressure (ICP) in critically ill patients.
Design: Systematic review and meta-analysis.
Data sources: Six databases, including Medline, EMBASE, and PubMed, from inception to 1 September 2018.
Study selection criteria: English language studies investigating accuracy of physical examination, imaging, or non-invasive tests among critically ill patients. The reference standard was ICP of 20 mm Hg or more using invasive ICP monitoring, or intraoperative diagnosis of raised ICP.
Data extraction: Two reviewers independently extracted data and assessed study quality using the quality assessment of diagnostic accuracy studies tool. Summary estimates were generated using a hierarchical summary receiver operating characteristic (ROC) model.
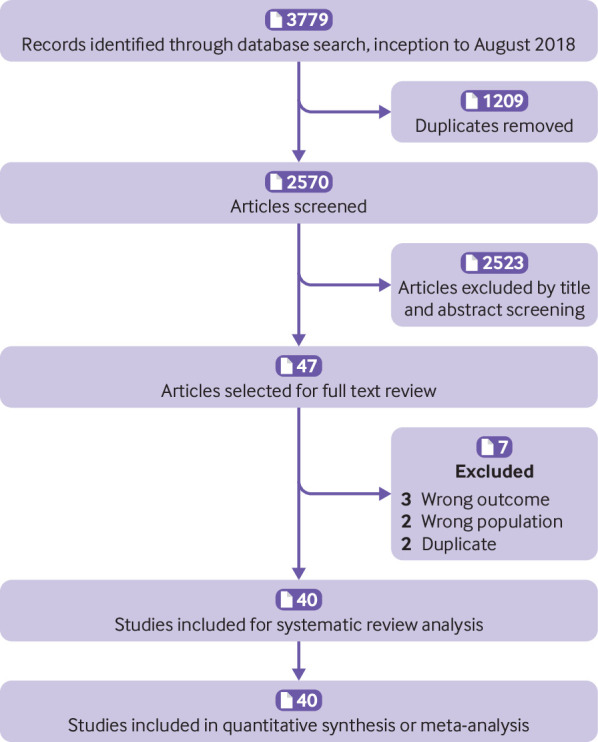
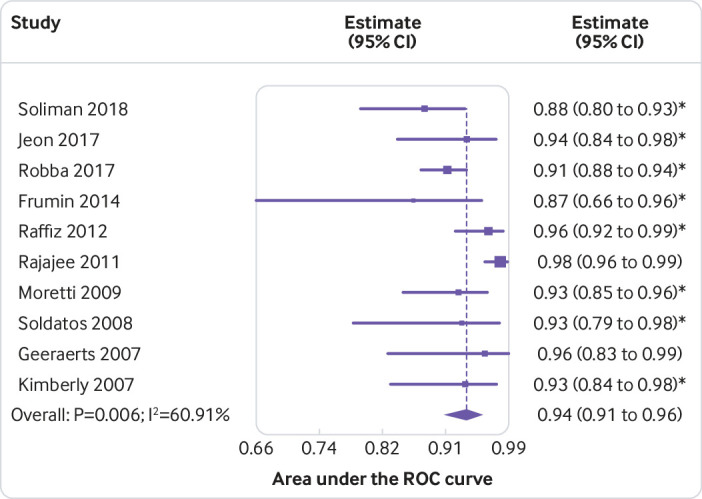
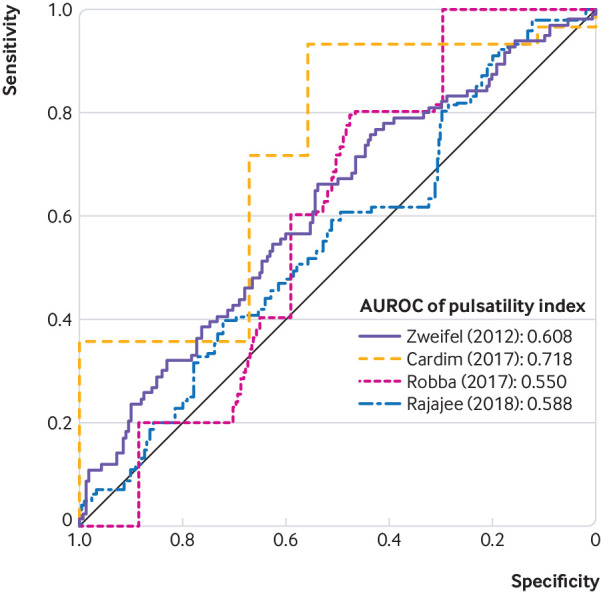
Results: 40 studies (n=5123) were included. Of physical examination signs, pooled sensitivity and specificity for increased ICP were 28.2% (95% confidence interval 16.0% to 44.8%) and 85.9% (74.9% to 92.5%) for pupillary dilation, respectively; 54.3% (36.6% to 71.0%) and 63.6% (46.5% to 77.8%) for posturing; and 75.8% (62.4% to 85.5%) and 39.9% (26.9% to 54.5%) for Glasgow coma scale of 8 or less. Among CT findings, sensitivity and specificity were 85.9% (58.0% to 96.4%) and 61.0% (29.1% to 85.6%) for compression of basal cisterns, respectively; 80.9% (64.3% to 90.9%) and 42.7% (24.0% to 63.7%) for any midline shift; and 20.7% (13.0% to 31.3%) and 89.2% (77.5% to 95.2%) for midline shift of at least 10 mm. The pooled area under the ROC (AUROC) curve for ONSD sonography was 0.94 (0.91 to 0.96). Patient level data from studies using TCD-PI showed poor performance for detecting raised ICP (AUROC for individual studies ranging from 0.55 to 0.72).
Conclusions: Absence of any one physical examination feature is not sufficient to rule out elevated ICP. Substantial midline shift could suggest elevated ICP, but the absence of shift cannot rule it out. ONSD sonography might have use, but further studies are needed. Suspicion of elevated ICP could necessitate treatment and transfer, regardless of individual non-invasive tests.
Registration: PROSPERO CRD42018105642.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Review: In critically ill adults, diagnostic accuracy of noninvasive tests for detecting elevated ICP varies.Ann Intern Med. 2019 Dec 17;171(12):JC68. doi: 10.7326/ACPJ201912170-068. Ann Intern Med. 2019. PMID: 31842226 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous