

Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis
- PMID: 31340984
- PMCID: PMC6651066
- DOI: 10.1136/bmj.l4363
Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis
Abstract
Objectives: To determine the rate of a first recurrent venous thromboembolism (VTE) event after discontinuation of anticoagulant treatment in patients with a first episode of unprovoked VTE, and the cumulative incidence for recurrent VTE up to 10 years.
Design: Systematic review and meta-analysis.
Data sources: Medline, Embase, and the Cochrane Central Register of Controlled Trials (from inception to 15 March 2019).
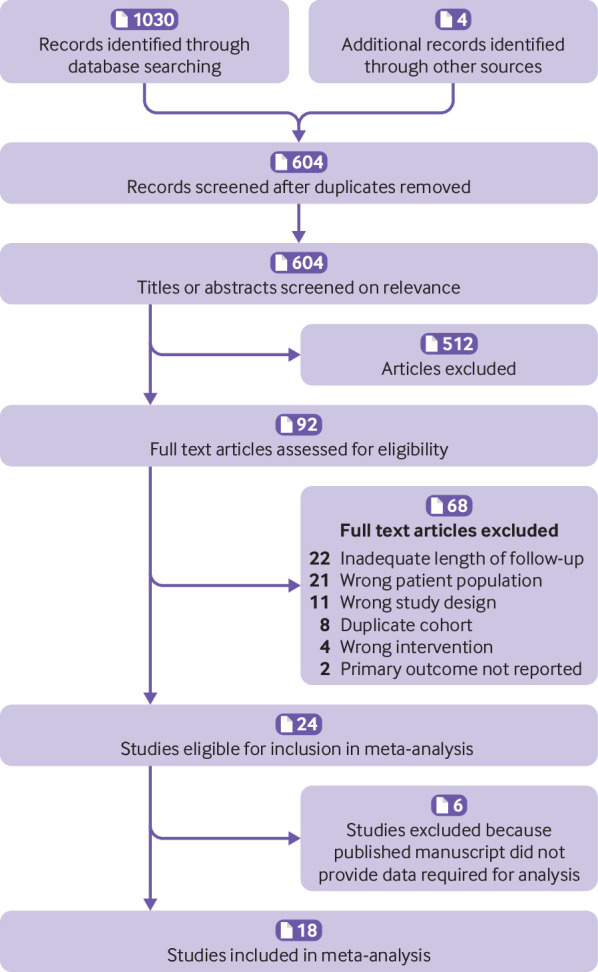
Study selection: Randomised controlled trials and prospective cohort studies reporting symptomatic recurrent VTE after discontinuation of anticoagulant treatment in patients with a first unprovoked VTE event who had completed at least three months of treatment.
Data extraction and synthesis: Two investigators independently screened studies, extracted data, and appraised risk of bias. Data clarifications were sought from authors of eligible studies. Recurrent VTE events and person years of follow-up after discontinuation of anticoagulant treatment were used to calculate rates for individual studies, and data were pooled using random effects meta-analysis. Sex and site of initial VTE were investigated as potential sources of between study heterogeneity.
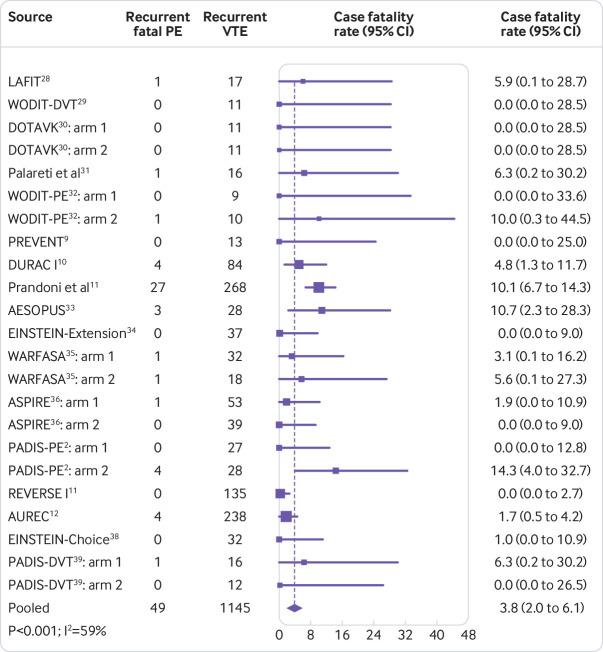
Results: 18 studies involving 7515 patients were included in the analysis. The pooled rate of recurrent VTE per 100 person years after discontinuation of anticoagulant treatment was 10.3 events (95% confidence interval 8.6 to 12.1) in the first year, 6.3 (5.1 to 7.7) in the second year, 3.8 events/year (95% confidence interval 3.2 to 4.5) in years 3-5, and 3.1 events/year (1.7 to 4.9) in years 6-10. The cumulative incidence for recurrent VTE was 16% (95% confidence interval 13% to 19%) at 2 years, 25% (21% to 29%) at 5 years, and 36% (28% to 45%) at 10 years. The pooled rate of recurrent VTE per 100 person years in the first year was 11.9 events (9.6 to 14.4) for men and 8.9 events (6.8 to 11.3) for women, with a cumulative incidence for recurrent VTE of 41% (28% to 56%) and 29% (20% to 38%), respectively, at 10 years. Compared to patients with isolated pulmonary embolism, the rate of recurrent VTE was higher in patients with proximal deep vein thrombosis (rate ratio 1.4, 95% confidence interval 1.1 to 1.7) and in patients with pulmonary embolism plus deep vein thrombosis (1.5, 1.1 to 1.9). In patients with distal deep vein thrombosis, the pooled rate of recurrent VTE per 100 person years was 1.9 events (95% confidence interval 0.5 to 4.3) in the first year after anticoagulation had stopped. The case fatality rate for recurrent VTE was 4% (95% confidence interval 2% to 6%).
Conclusions: In patients with a first episode of unprovoked VTE who completed at least three months of anticoagulant treatment, the risk of recurrent VTE was 10% in the first year after treatment, 16% at two years, 25% at five years, and 36% at 10 years, with 4% of recurrent VTE events resulting in death. These estimates should inform clinical practice guidelines, enhance confidence in counselling patients of their prognosis, and help guide decision making about long term management of unprovoked VTE.
Systematic review registration: PROSPERO CRD42017056309.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: MC has received grants from Leo Pharma, Bristol-Myers Squibb, Bayer, Octapharma, personal fees from Sanofi Aventis, Pfizer, Boehringer Ingelheim, Leo Pharma, Bayer Pfizer, Servier, and been on the advisory board for Leo Pharma and Sanofi Aventis, outside the submitted work; CK has received grants from Bayer, outside the submitted work. JIW has received personal fees from Bayer, Boehringer Ingelheim, Bristol Myers Squibb Daiichi-Sankyo, Ionis Pharmaceuticals, Janssen, Merck, Pfizer, and Portola, outside the submitted work; SS has received grants from Boehringer Ingelheim and Octapharma, personal fees from Boehringer Ingelheim, Bayer, Daiichi Sankyo, Octapharma, Sanofi, Alnylam, and Bristol-Myers-Squibb, outside the submitted work; FC has received grants from Pfizer, and personal fees from Bayer, BMS, Aztra Zeneca, leopharma, outside the submitted work; CB has received personal fees from Bayer HealthCare, Daiichi Sankyo, Bristol Myers Squibb, and Servier, outside the submitted work; GA has received personal fees from Bristol-Myers-Squibb, Bayer Healthcare, Boehringer Ingelheim, and Daiichi Sankyo, outside the submitted work; AWAL reports being an employee of Bayer HealthCare; MHP has received personal fees from Pfizer and Daiichi Sankyo, outside the submitted work; BH reports past research from Cornerstone Research Group for methodologic advice related to the conduct of systematic reviews and meta-analysis, outside the submitted work; GP has received personal fees from Alfasigma, Pfizer, BMS, Roche, and Werfen, outside the submitted work. There are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Minimizing recurrent venous thromboembolism.BMJ. 2019 Jul 25;366:l4686. doi: 10.1136/bmj.l4686. BMJ. 2019. PMID: 31345836 No abstract available.
References
-
- Boutitie F, Pinede L, Schulman S, et al. Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants’ data from seven trials. BMJ 2011;342:d3036. 10.1136/bmj.d3036 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases