

The Underlying Stroke Etiology: A Comparison of Two Classifications in a Rural Setup
- PMID: 31341751
- PMCID: PMC6639087
- DOI: 10.7759/cureus.5157
The Underlying Stroke Etiology: A Comparison of Two Classifications in a Rural Setup
Abstract
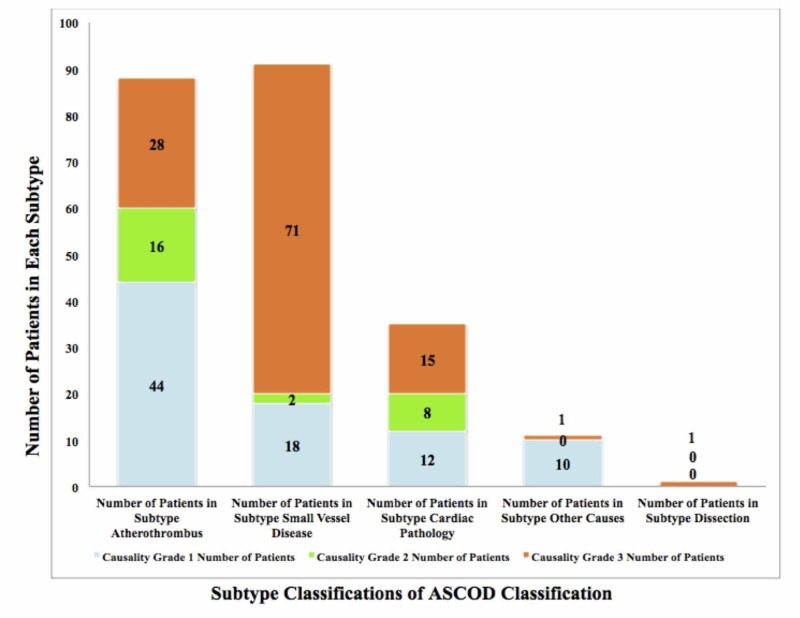
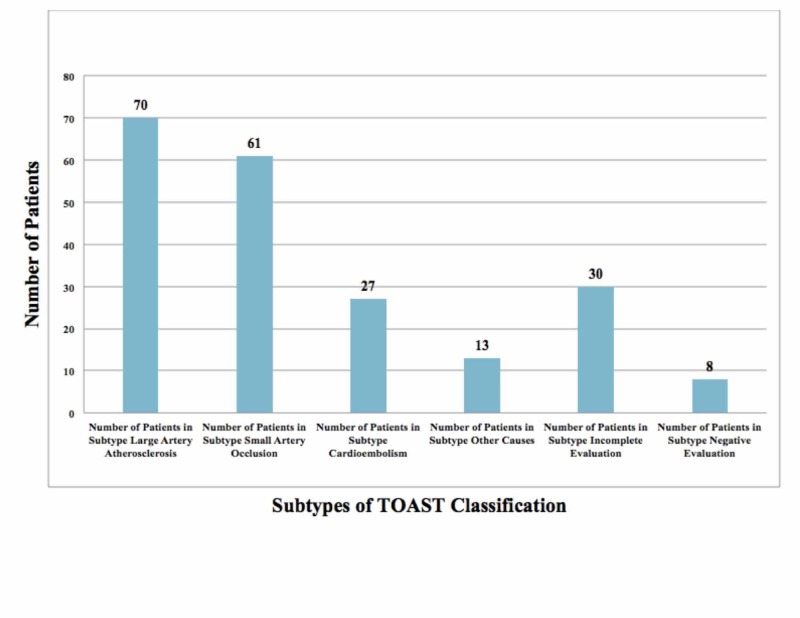
Introduction This study compares the Trial of Org 10172 in Acute Stroke Treatment (TOAST) and the atherothrombosis, small vessel disease, cardiac pathology, other causes, and dissection (ASCOD) classification performed in a rural hospital setup. Stroke is the second leading cause of death after ischemic heart disease with over 9.5 million new cases of ischemic stroke in 2016. Stroke is a complex disease with numerous contributing factors. India needs a standardized stroke classification system, as without one it becomes difficult to collect data on stroke patients, perform follow-ups, and provide appropriate secondary prevention. A standardized stroke classification system would also help in building a nationwide database in order to note epidemiological trends of ischemic stroke. This would also create greater awareness regarding stroke in rural parts of India where healthcare is difficult to access. Aims and objectives Our aim was to review all admitted stroke patients' data and classify their etiology and mechanism based on the TOAST and ASCOD classification systems. The ASCOD classification has yet to be utilized in the Indian population. The two classifications are then compared in order to gain a better insight into which classification is a better fit for the Indian population. Both are based on the etiology of ischemic stroke but the ASCOD classification differs because it gives suitable secondary prevention measures based on the diseases linked to stroke. ASCOD also gives a proper indication of the patient's present causative factor (similar to TOAST) and other factors that can possibly lead to further recurrences. This is different from TOAST, which denotes only a single cause for stroke and eliminates the possibility of other involved contributing factors. Materials and methods All patients involved in the study were admitted to a rural Indian hospital from January 2014 to July 2016. All the relevant clinical details of each patient were then retrieved from the hospital's electronic medical record system for the study. We then classified all the patients based on the TOAST and ASCOD classification criteria. Results Using the ASCOD classification, we found that 179 (86%) patients out of 209 had either atherothrombosis or small vessel disease. The ASCOD classification also showed substantial evidence that the determined stroke mechanism/etiology is interconnected to multiple causal factors in over 50% of patients. In contrast, the TOAST classification had identified a larger number of ischemic stroke patients as having an etiology of other and undetermined causes as compared to the ASCOD classification. Conclusion The ASCOD classification is better to use in patients and helps decide the secondary prevention appropriately.
Keywords: ascod classification; atherothrombosis; cardiac pathology; dissection; hypertension; ischemic stroke; other causes; rural healthcare; small vessel disease; toast classification.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cerebrovascular disease in the community: results of a WHO collaborative study. Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2395897/ Bull World Health Organ. 1980;58:113–130. - PMC - PubMed
-
- A prospective community-based study of stroke in Kolkata, India. Das SK, Banerjee TK, Biswas A, et al. Stroke. 2007;38:906–910. - PubMed
-
- Global burden of stroke. Katan M, Luft A. Semin Neurol. 2018;38:208–211. - PubMed
LinkOut - more resources
Full Text Sources