

City-wide electronic health records reveal gender and age biases in administration of known drug-drug interactions
- PMID: 31341958
- PMCID: PMC6650500
- DOI: 10.1038/s41746-019-0141-x
City-wide electronic health records reveal gender and age biases in administration of known drug-drug interactions
Abstract
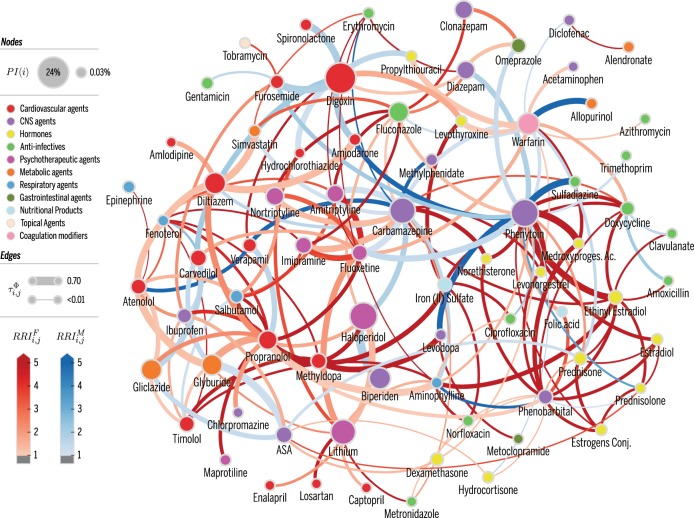
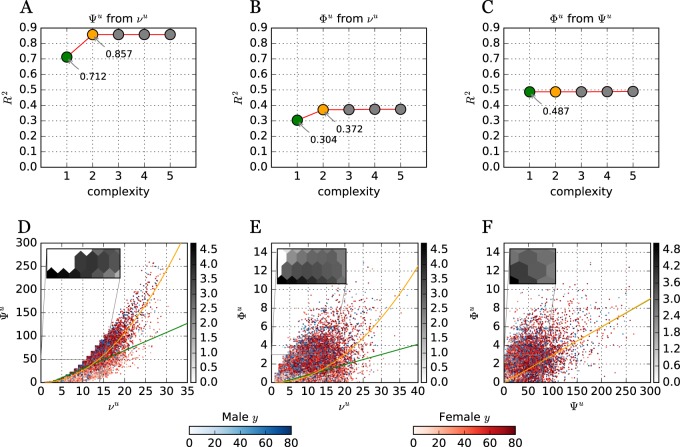
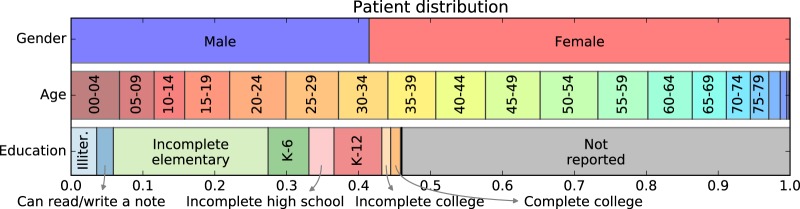
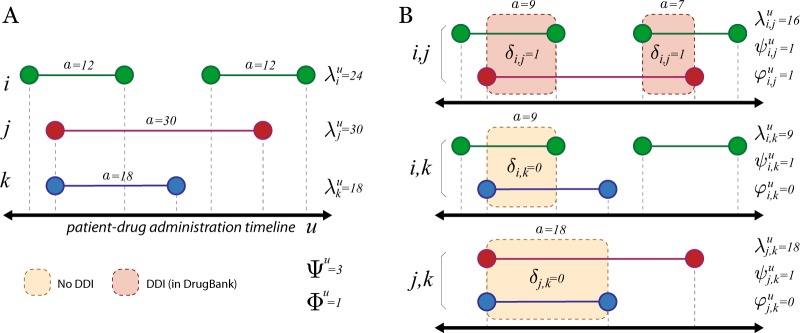
The occurrence of drug-drug-interactions (DDI) from multiple drug dispensations is a serious problem, both for individuals and health-care systems, since patients with complications due to DDI are likely to reenter the system at a costlier level. We present a large-scale longitudinal study (18 months) of the DDI phenomenon at the primary- and secondary-care level using electronic health records (EHR) from the city of Blumenau in Southern Brazil (pop. ≈340,000). We found that 181 distinct drug pairs known to interact were dispensed concomitantly to 12% of the patients in the city's public health-care system. Further, 4% of the patients were dispensed drug pairs that are likely to result in major adverse drug reactions (ADR)-with costs estimated to be much larger than previously reported in smaller studies. The large-scale analysis reveals that women have a 60% increased risk of DDI as compared to men; the increase becomes 90% when considering only DDI known to lead to major ADR. Furthermore, DDI risk increases substantially with age; patients aged 70-79 years have a 34% risk of DDI when they are dispensed two or more drugs concomitantly. Interestingly, a statistical null model demonstrates that age- and female-specific risks from increased polypharmacy fail by far to explain the observed DDI risks in those populations, suggesting unknown social or biological causes. We also provide a network visualization of drugs and demographic factors that characterize the DDI phenomenon and demonstrate that accurate DDI prediction can be included in health care and public-health management, to reduce DDI-related ADR and costs.
Keywords: Computational science; Drug regulation; Epidemiology; Public health; Risk factors.
Conflict of interest statement
Competing interestsThe authors declare no competing interests.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
