

Adaptive radiotherapy: The Elekta Unity MR-linac concept
- PMID: 31341976
- PMCID: PMC6630157
- DOI: 10.1016/j.ctro.2019.04.001
Adaptive radiotherapy: The Elekta Unity MR-linac concept
Abstract
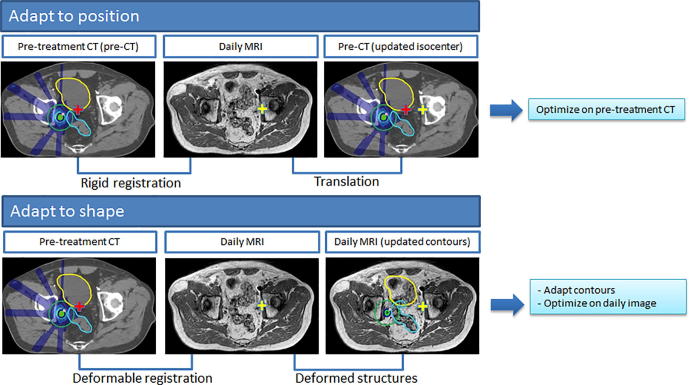
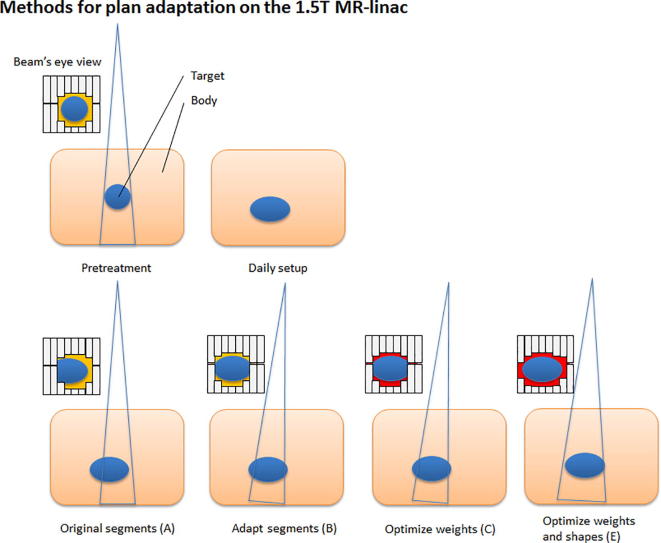
Background and purpose: The promise of the MR-linac is that one can visualize all anatomical changes during the course of radiotherapy and hence adapt the treatment plan in order to always have the optimal treatment. Yet, there is a trade-off to be made between the time spent for adapting the treatment plan against the dosimetric gain. In this work, the various daily plan adaptation methods will be presented and applied on a variety of tumour sites. The aim is to provide an insight in the behavior of the state-of-the-art 1.5 T MRI guided on-line adaptive radiotherapy methods.
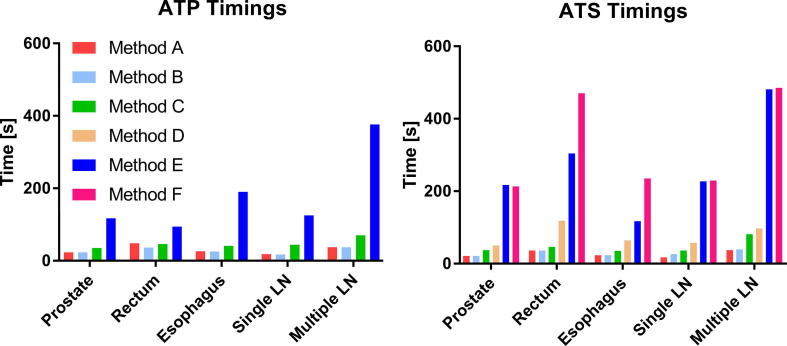
Materials and methods: To explore the different available plan adaptation workflows and methods, we have simulated online plan adaptation for five cases with varying levels of inter-fraction motion, regions of interest and target sizes: prostate, rectum, esophagus and lymph node oligometastases (single and multiple target). The plans were evaluated based on the clinical dose constraints and the optimization time was measured.
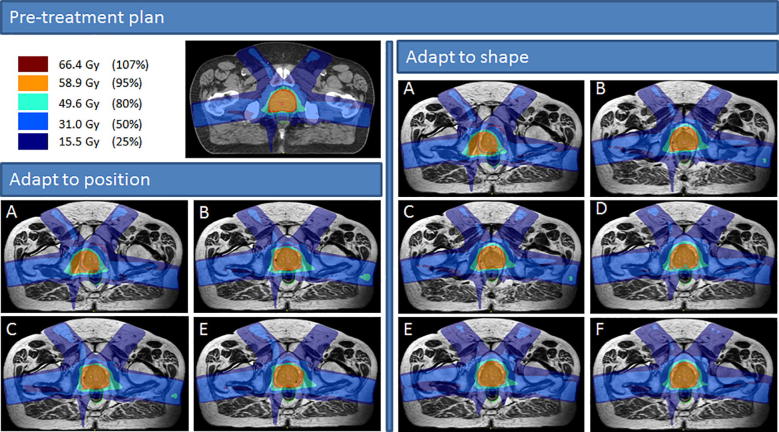
Results: The time needed for plan adaptation ranged between 17 and 485 s. More advanced plan adaptation methods generally resulted in more plans that met the clinical dose criteria. Violations were often caused by insufficient PTV coverage or, for the multiple lymph node case, a too high dose to OAR in the vicinity of the PTV. With full online replanning it was possible to create plans that met all clinical dose constraints for all cases.
Conclusion: Daily full online replanning is the most robust adaptive planning method for Unity. It is feasible for specific sites in clinically acceptable times. Faster methods are available, but before applying these, the specific use cases should be explored dosimetrically.
Keywords: Adaptive radiotherapy; MR-linac; MRI-guided radiotherapy; Online plan adaptation; Radiotherapy.
Figures
References
-
- Lagendijk J.J.W., Raaymakers B.W., van Vulpen M. The magnetic resonance imaging-linac system. Semin Radiat Oncol. 2014;24:207–209. - PubMed
-
- Raaymakers B.W., Jürgenliemk-Schulz I.M., Bol G.H., Glitzner M., Kotte A.N.T.J., van Asselen B. First patients treated with a 1.5 T MRI-Linac: clinical proof of concept of a high-precision, high-field MRI guided radiotherapy treatment. Phys Med Biol. 2017;62:L41–L50. - PubMed
-
- Raaymakers B.W., Lagendijk J.J.W., Overweg J., Kok J.G., Raaijmakers A.J., Kerkhof E.M. Integrating a 1.5 T MRI scanner with a 6 MV accelerator: proof of concept. Phys Med Biol. 2009;54:N229–N237. - PubMed
-
- Werensteijn-Honingh A.M., Kroon P.S., Winkel D., Aalbers E.M., Van Asselen B., Bol G.H. Feasibility of stereotactic radiotherapy using a 1.5 T MR-linac: multi-fraction treatment of pelvic lymph node oligometastases. Radiother Oncol. 2019;134:50–54. - PubMed
-
- Kleijnen J.J.E., van Asselen B., Burbach J.P.M., Intven M.P.W., Philippens M.E.P., Reerink O. Evolution of motion uncertainty in rectal cancer: implications for adaptive radiotherapy. Phys Med Biol. 2016;61:1–11. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
