

Use of Cell Cycle Arrest Biomarkers in Conjunction With Classical Markers of Acute Kidney Injury
- PMID: 31343478
- PMCID: PMC6750148
- DOI: 10.1097/CCM.0000000000003907
Use of Cell Cycle Arrest Biomarkers in Conjunction With Classical Markers of Acute Kidney Injury
Abstract
Objectives: Decreased urine output and/or increased serum creatinine may herald the development of acute kidney injury or reflect normal physiology. In this secondary analysis of the Sapphire study, we examined biomarkers of cell cycle arrest in the settings of oliguria and/or azotemia to improve risk assessment when used with conventional indices in predicting severe acute kidney injury (Kidney Disease: Improving Global Outcomes 3 defined by the need for renal replacement therapy or changes in urine output, serum creatinine or both) or death.
Design: Prospective, international, Sapphire study.
Setting: Academic Medical Center.
Patients: Patients without acute kidney injury Kidney Disease: Improving Global Outcomes stage 2 or 3.
Interventions: None.
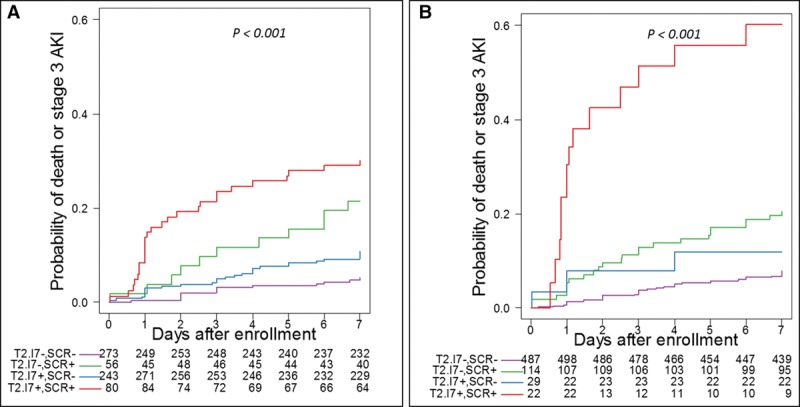
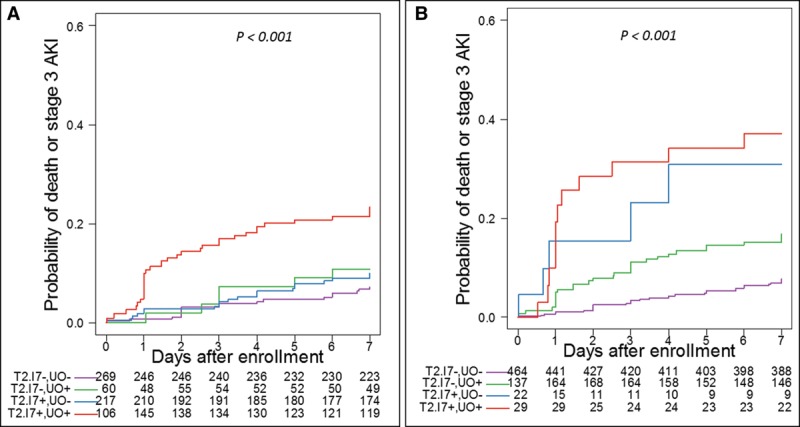
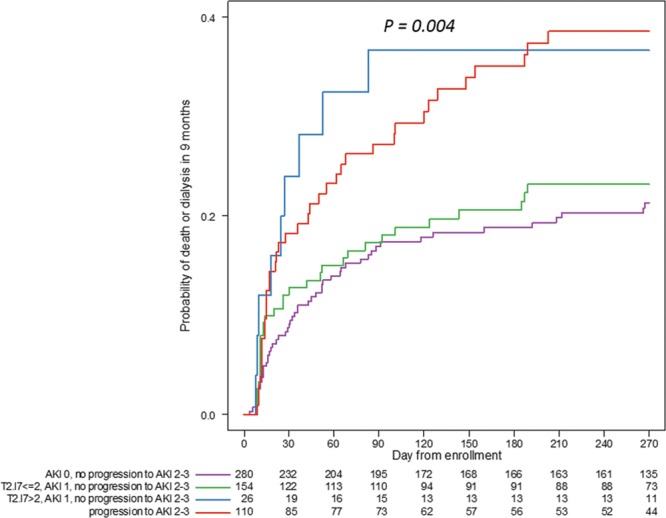
Measurements and main results: The primary endpoint being development of severe acute kidney injury or death within 1 week. Secondary analysis examined the relationship between tissue inhibitor of metalloproteinases-2 ([TIMP-2]) and insulin growth factor binding protein 7 ([IGFBP7]) and 9-month death or dialysis conditioned on progression to stage 2-3 acute kidney injury within 1 week. Seventy-nine patients reached the primary endpoint and were more likely to be surgical, with higher nonrenal Acute Physiology and Chronic Health Evaluation III scores and more chronic kidney disease. Stage 1 urine output, serum creatinine, and urinary [TIMP-2]•[IGFBP7] greater than 2.0 were all predictive of progression to the primary endpoint independent from nonrenal Acute Physiology and Chronic Health Evaluation III score. Combinations of predictors increased the hazard ratios considerably (from 2.17 to 4.14 to 10.05, respectively). In the presence of acute kidney injury (stage 1), [TIMP-2]•[IGFBP7] greater than 2.0 leads to an increased risk of death or dialysis at 9 months even in the absence of progression of acute kidney injury (stage 2-3) within 7 days.
Conclusions: Cell cycle arrest biomarkers, TIMP-2 and IGFBP7, improve risk stratification for severe outcomes in patients with stage 1 acute kidney injury by urine output, serum creatinine or both, with risk increasing with each acute kidney injury indicator. Longer term outcomes demonstrate that the associated risks of a [TIMP-2]•[IGFBP7] greater than 2.0 is equivalent to acute kidney injury progression even where no progression from stage 1 acute kidney injury is observed.
Figures
References
-
- Bellomo R, Kellum J, Ronco C. Acute renal failure: Time for consensus. Intensive Care Med 2001; 27:1685–1688 - PubMed
-
- Hoste EA, Kellum JA. Acute kidney injury: Epidemiology and diagnostic criteria. Curr Opin Crit Care 2006; 12:531–537 - PubMed
-
- Petäjä L, Vaara S, Liuhanen S, et al. Acute kidney injury after cardiac surgery by complete KDIGO criteria predicts increased mortality. J Cardiothorac Vasc Anesth 2017; 31:827–836 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
