

Emphysema phenotypes and lung cancer risk
- PMID: 31344121
- PMCID: PMC6657833
- DOI: 10.1371/journal.pone.0219187
Emphysema phenotypes and lung cancer risk
Abstract
Background: To assess the relationship between lung cancer and emphysema subtypes.
Objective: Airflow obstruction and emphysema predispose to lung cancer. Little is known, however, about the lung cancer risk associated with different emphysema phenotypes. We assessed the risk of lung cancer based on the presence, type and severity of emphysema, using visual assessment.
Methods: Seventy-two consecutive lung cancer cases were selected from a prospective cohort of 3,477 participants enrolled in the Clínica Universidad de Navarra's lung cancer screening program. Each case was matched to three control subjects using age, sex, smoking history and body mass index as key variables. Visual assessment of emphysema and spirometry were performed. Logistic regression and interaction model analysis were used in order to investigate associations between lung cancer and emphysema subtypes.
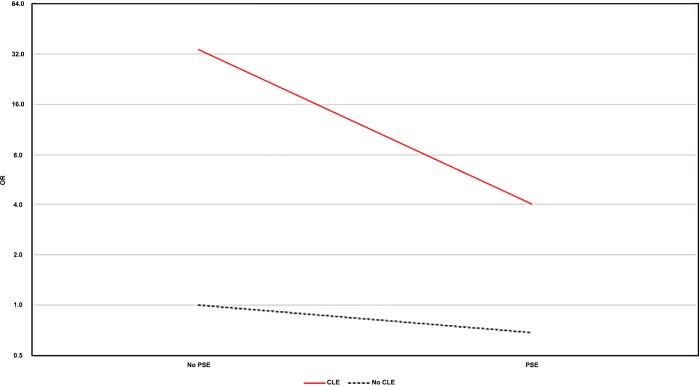
Results: Airflow obstruction and visual emphysema were significantly associated with lung cancer (OR = 2.8, 95%CI: 1.6 to 5.2; OR = 5.9, 95%CI: 2.9 to 12.2; respectively). Emphysema severity and centrilobular subtype were associated with greater risk when adjusted for confounders (OR = 12.6, 95%CI: 1.6 to 99.9; OR = 34.3, 95%CI: 25.5 to 99.3, respectively). The risk of lung cancer decreases with the added presence of paraseptal emphysema (OR = 4.0, 95%CI: 3.6 to 34.9), losing this increased risk of lung cancer when it occurs alone (OR = 0.7, 95%CI: 0.5 to 2.6).
Conclusions: Visual scoring of emphysema predicts lung cancer risk. The centrilobular phenotype is associated with the greatest risk.
Conflict of interest statement
All authors have read the journal's authorship agreement and policy on disclosure of potential conflicts of interest. JJZ is a part-time employee of VisionGate, Inc. JPd-T has received consultancy fees for participating in advisory boards for Takeda Pharmaceuticals International GmbH, Menarini, and Novartis AG; he also received fees for speaking activities from GlaxoSmithKline plc, AstraZeneca, Chiesi, Menarini, Novartis AG, Merck, Sharp & Dohme Corporation, and Takeda Pharmaceuticals International GmbH. DFY is a named inventor on a number of patents and patent applications relating to the evaluation of diseases of the chest including measurement of nodules. Some of these, which are owned by Cornell Research Foundation (CRF), are non-exclusively licensed to General Electric. As an inventor of these patents, DFY is entitled to a share of any compensation which CRF may receive from its commercialization of these patents. He is also an equity owner in Accumetra, a privately held technology company committed to improving the science and practice of image-based decision making. DFY also serves on the advisory board of GRAIL. CIH is the President and serves on the board of the Early Diagnosis and Treatment Research Foundation. She receives no compensation from the Foundation. CIH is also a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell Research Foundation (CRF). Since 2009, CIH does not accept any financial benefit from these patents including royalties and any other proceeds related to the patents or patent applications owned by CRF. APR holds shares in VisionGate Inc., is owner of D4Vision Inc., and receives royalties from patents owned and licensed by Cornell Research Foundation. All other authors have no competing interests to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
