

Role of chemotherapy in 5000 patients with head and neck cancer treated by curative surgery: A subgroup analysis of the meta-analysis of chemotherapy in head and neck cancer
- PMID: 31345376
- PMCID: PMC7029787
- DOI: 10.1016/j.oraloncology.2019.06.001
Role of chemotherapy in 5000 patients with head and neck cancer treated by curative surgery: A subgroup analysis of the meta-analysis of chemotherapy in head and neck cancer
Abstract
Objective: To evaluate the effect of chemotherapy added to a surgical locoregional treatment (LRT) for patients with locally advanced head and neck squamous cell carcinoma (HNSCC).
Materials and methods: We studied the sub-group of trials with surgical LRT included in the meta-analysis on chemotherapy in head and neck cancer (MACH-NC). Data from published and unpublished randomized trials comparing the addition of chemotherapy to LRT in HNSCC patients were sought using electronic database searching for the period 1965-2000, hand searching and by contacting experts in the field. Trials with less than 60 patients, or preoperative radiotherapy or where the type of LRT could not be individually determined were excluded. All individual patient data were checked for internal consistency, compared with published reports, and validated with trialists. Data were pooled using a fixed-effect model. Heterogeneity was assessed using Cochrane test and I2 statistic.
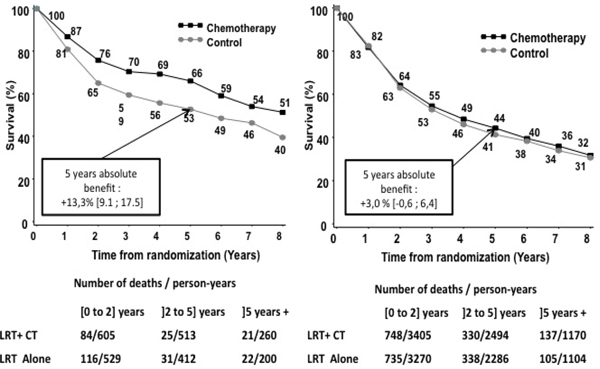
Results: Twenty-four trials were eligible (5000 patients). Chemotherapy improved overall survival (HR = 0.92 [95%CI: 0.85-0.99] p = 0.02). There was a significant interaction between treatment effect and timing of chemotherapy (p = 0.08 at pre-specified threshold of 0.10) with a greater effect for concomitant chemotherapy (HR = 0.79, 95%CI: 0.69-0.92). The benefit of chemotherapy was greater in women (HRwomen = 0.63, 95%CI: 0.50-0.80) compared to men (HRmen = 0.96, 95%CI: 0.89-1.04; p for interaction = 0.001).
Conclusions: This analysis confirmed the benefit of concomitant chemotherapy added to surgical LRT. The role of induction therapy as yet to be determined as it did not improve OS. Women may benefit more than men from chemotherapy.
Keywords: Chemotherapy; Head and neck cancer; Individual patient data; Meta-analysis; Randomized trial; Squamous cell carcinoma; Surgery.
Copyright © 2019. Published by Elsevier Ltd.
Conflict of interest statement
Conflict Of Interest statement
None declared
Figures




Comment in
-
Response to R. Jayaraj.Oral Oncol. 2020 Mar;102:104439. doi: 10.1016/j.oraloncology.2019.104439. Epub 2019 Nov 2. Oral Oncol. 2020. PMID: 31685291 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
