

Early Clinical Infancy Outcomes for Microcephaly and/or Small for Gestational Age Zika-Exposed Infants
- PMID: 31346616
- PMCID: PMC7286378
- DOI: 10.1093/cid/ciz704
Early Clinical Infancy Outcomes for Microcephaly and/or Small for Gestational Age Zika-Exposed Infants
Abstract
Background: Zika-exposed infants with microcephaly (proportional or disproportional) and those who are small for gestational age without microcephaly should be closely followed, particularly their growth trajectories. They are at high risk of adverse outcomes in the first year of life.Antenatal Zika virus (ZIKV) exposure may lead to adverse infant outcomes including microcephaly and being small for gestational age (SGA). ZIKV-exposed infants with a diagnosis of microcephaly (proportional [PM] or disproportional [DM]) or SGA at birth were evaluated with anthropometric measurements and health outcomes.
Methods: Infants had laboratory-confirmed ZIKV exposure in Brazil. PM, DM, or SGA classification was based on head circumference and weight. First-year growth parameters and clinical outcomes were recorded with analyses performed.
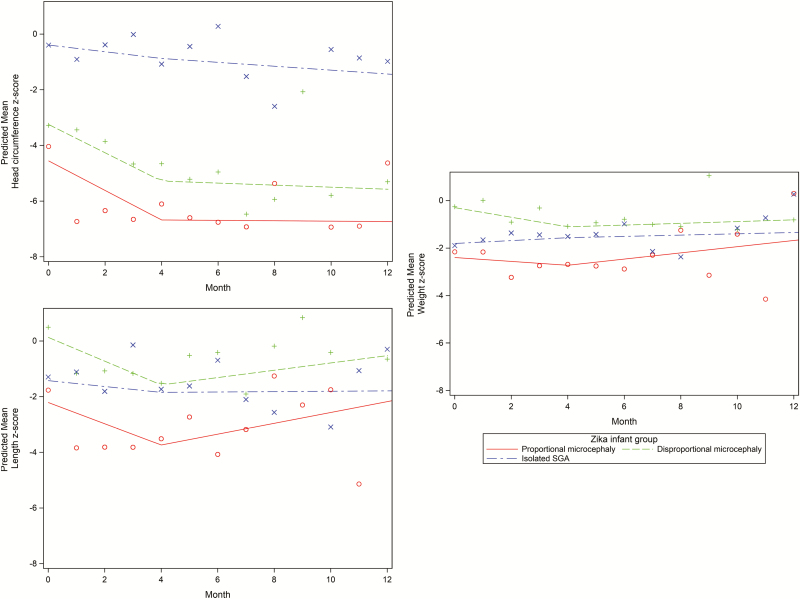
Results: Among the 156 ZIKV-exposed infants, 14 (9.0%) were SGA, 13 (8.3%) PM, 13 (8.3%) DM, and 116 (74.4%) were neither SGA nor had microcephaly (NSNM). High rates of any neurologic, ophthalmologic, and hearing abnormalities were observed for PM (100%), DM (100%), and SGA (42.9%) vs NSNM infants (18.3%; P <.001); odds ratio [OR], 3.4 (95% confidence interval [CI], 1.1-10.7) for SGA vs NSNM. Neuroimaging abnormalities were seen in 100% of PM and DM and in 42.9% of SGA vs NSNM infants 16%; (P <.001); OR 3.9 (95% CI, 1.2-12.8) for SGA vs NSNM. Growth rates by z score, particularly for microcephaly infants, were poor after birth but showed improvement beyond 4 months of life.
Conclusions: ZIKV-exposed infants with microcephaly (PM and DM) had similarly high rates of adverse outcomes but showed improvement in growth measurements beyond 4 months of life. While SGA infants had fewer adverse outcomes compared with microcephaly infants, notable adverse outcomes were observed in some; their odds of having adverse outcomes were 3 to 4 times greater compared to NSNM infants.Zika-exposed infants with microcephaly, irrespective of being proportional or disproportional, and those who are small for gestational age without microcephaly should be closely followed, particularly their growth trajectories. They are at high risk of adverse outcomes in the first year of life.
Keywords: Zika; congenital Zika syndrome; microcephaly; proportional microcephaly; small for gestational age (SGA).
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Zika, the Newest TORCH Infectious Disease in the Americas.Clin Infect Dis. 2020 Jun 10;70(12):2673-2674. doi: 10.1093/cid/ciz709. Clin Infect Dis. 2020. PMID: 31346608 No abstract available.
References
-
- PAHO WHO. Regional Zika epidemiological update (Americas) 2016.
-
- PAHO WHO. Zika suspected and confirmed cases reported by countries and territories in the Americas Cumulative cases, 2015–2016 Available at: http://www.paho.org/hq/index.php?option=com_docman&task=doc_view&Itemid=....
-
- PAHO WHO. Zika cases and congenital syndrome associated with Zika virus reported by countries and territories in the Americas, 2015–12017: cumulative cases 2017.
