

The diagnostic accuracy for ARDS of global versus regional lung ultrasound scores - a post hoc analysis of an observational study in invasively ventilated ICU patients
- PMID: 31346914
- PMCID: PMC6658630
- DOI: 10.1186/s40635-019-0241-6
The diagnostic accuracy for ARDS of global versus regional lung ultrasound scores - a post hoc analysis of an observational study in invasively ventilated ICU patients
Abstract
Background: Semi-quantification of lung aeration by ultrasound helps to assess presence and extent of pulmonary pathologies, including the acute respiratory distress syndrome (ARDS). It is uncertain which lung regions add most to the diagnostic accuracy for ARDS of the frequently used global lung ultrasound (LUS) score. We aimed to compare the diagnostic accuracy of the global versus those of regional LUS scores in invasively ventilated intensive care unit patients.
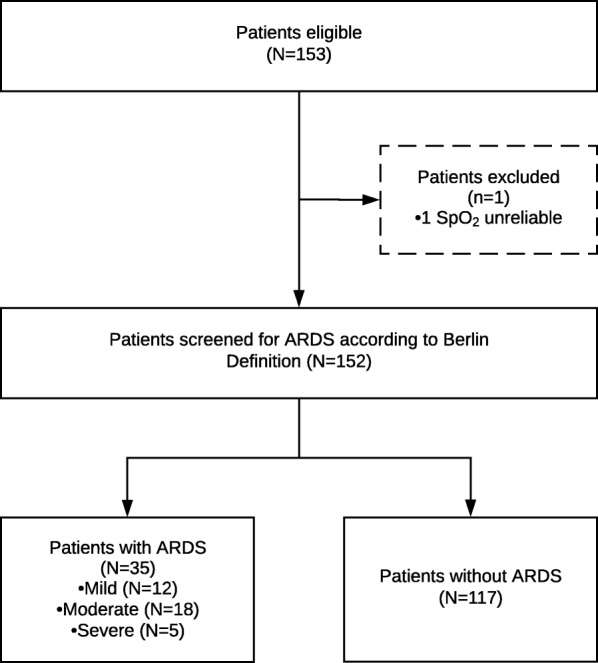
Methods: This was a post-hoc analysis of a single-center observational study in the mixed medical-surgical intensive care unit of a university-affiliated hospital in the Netherlands. Consecutive patients, aged ≥ 18 years, and are expected to receive invasive ventilation for > 24 h underwent a LUS examination within the first 2 days of ventilation. The Berlin Definition was used to diagnose ARDS, and to classify ARDS severity. From the 12-region LUS examinations, the global score (minimum 0 to maximum 36) and 3 regional scores (the 'anterior,' 'lateral,' and 'posterior' score, minimum 0 to maximum 12) were computed. The area under the receiver operating characteristic (AUROC) curve was calculated and the best cutoff for ARDS discrimination was determined for all scores.
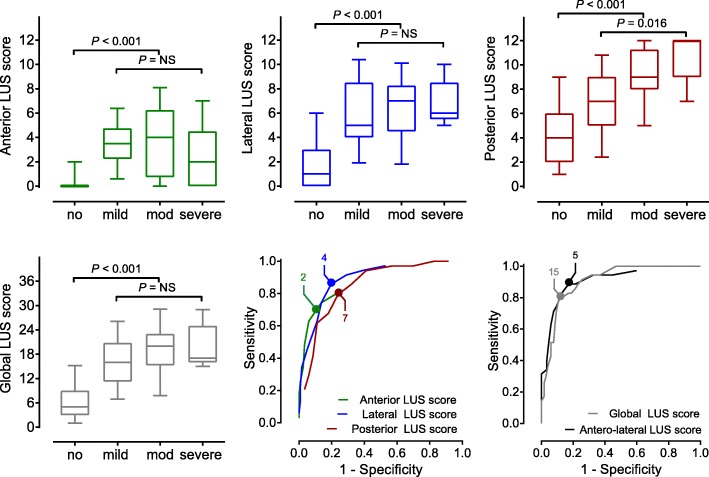
Results: The study enrolled 152 patients; 35 patients had ARDS. The global score was higher in patients with ARDS compared to patients without ARDS (median 19 [15-23] vs. 5 [3-9]; P < 0.001). The posterior score was the main contributor to the global score, and was the only score that increased significantly with ARDS severity. However, the posterior score performed worse than the global score in diagnosing ARDS, and it had a positive predictive value of only 50 (41-59)% when using the optimal cutoff. The combined anterolateral score performed as good as the global score (AUROC of 0.91 [0.85-0.97] vs. 0.91 [0.86-0.95]).
Conclusions: While the posterior score increases with ARDS severity, its diagnostic accuracy for ARDS is hampered due to an unfavorable signal-to-noise ratio. An 8-region 'anterolateral' score performs as well as the global score and may prove useful to exclude ARDS in invasively ventilated ICU patients.
Keywords: ARDS; Diagnosis; Diagnostic accuracy; Intensive care; Lung ultrasound; Ventilation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
