

Human foveal cone photoreceptor topography and its dependence on eye length
- PMID: 31348002
- PMCID: PMC6660219
- DOI: 10.7554/eLife.47148
Human foveal cone photoreceptor topography and its dependence on eye length
Abstract
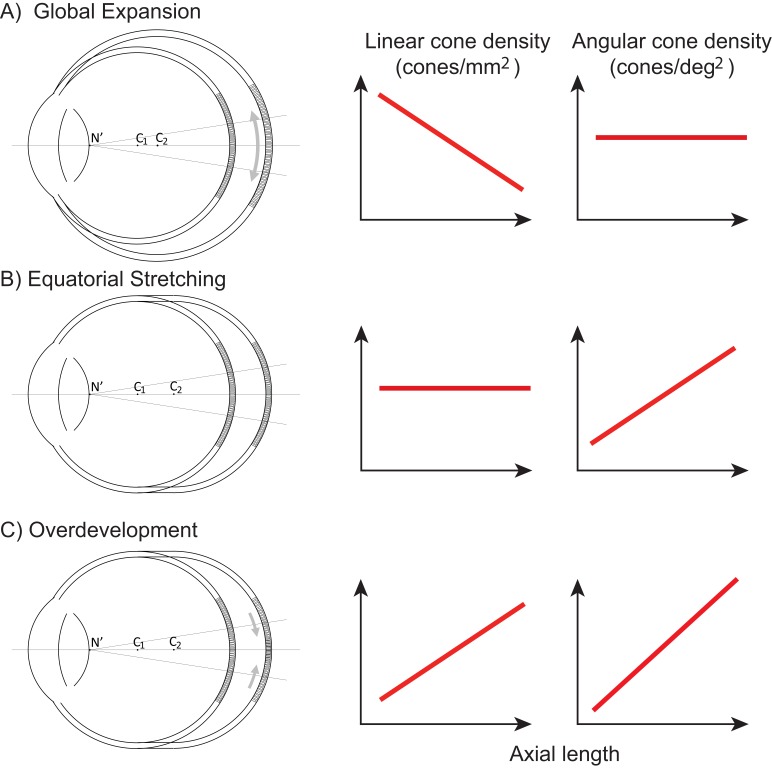
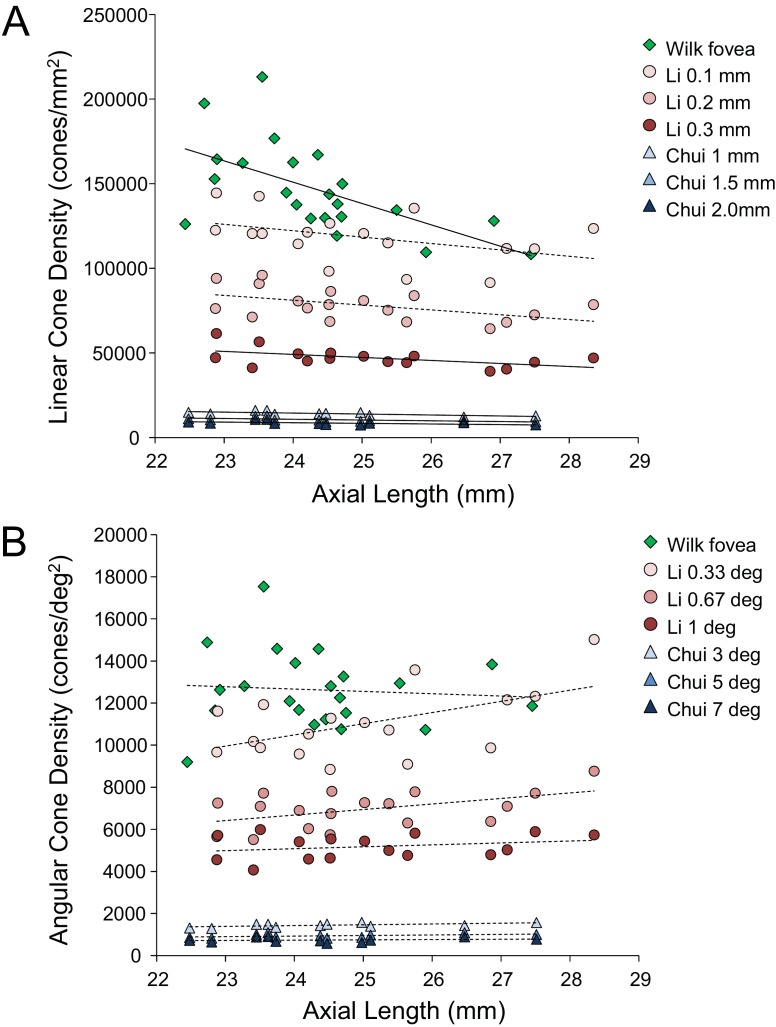
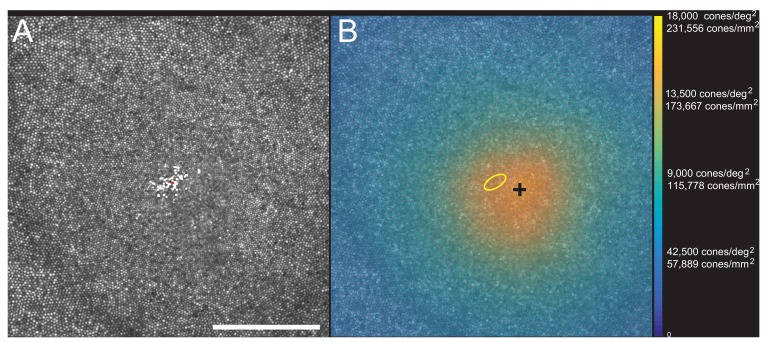
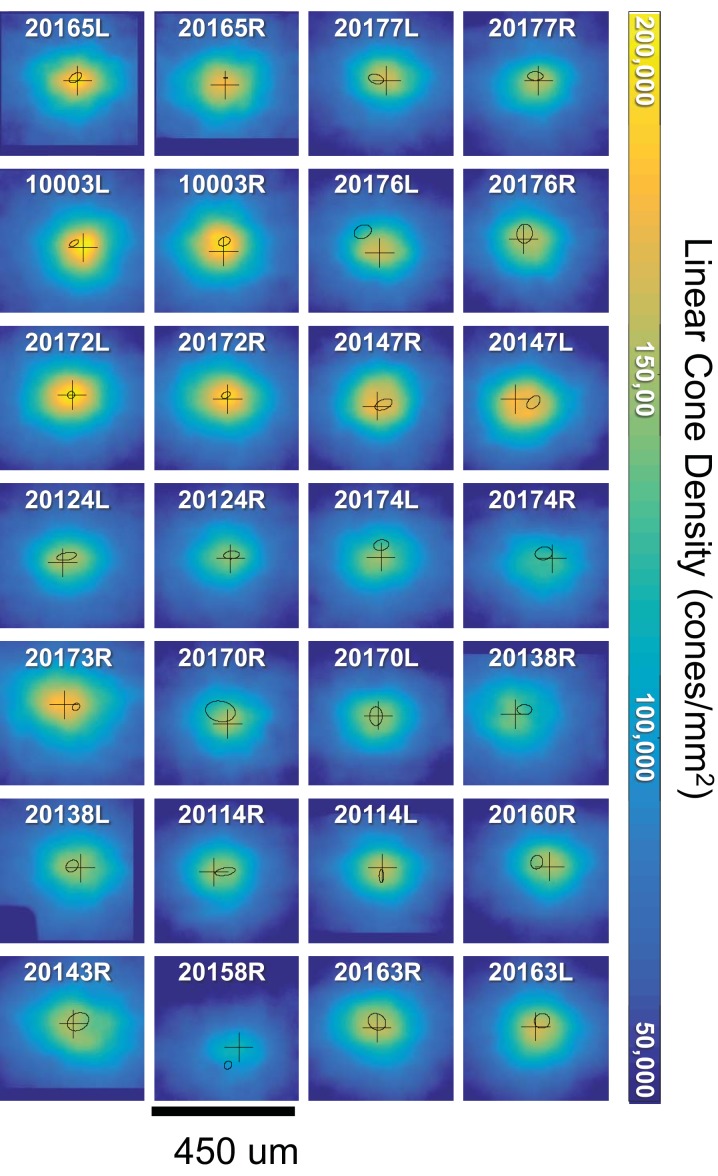
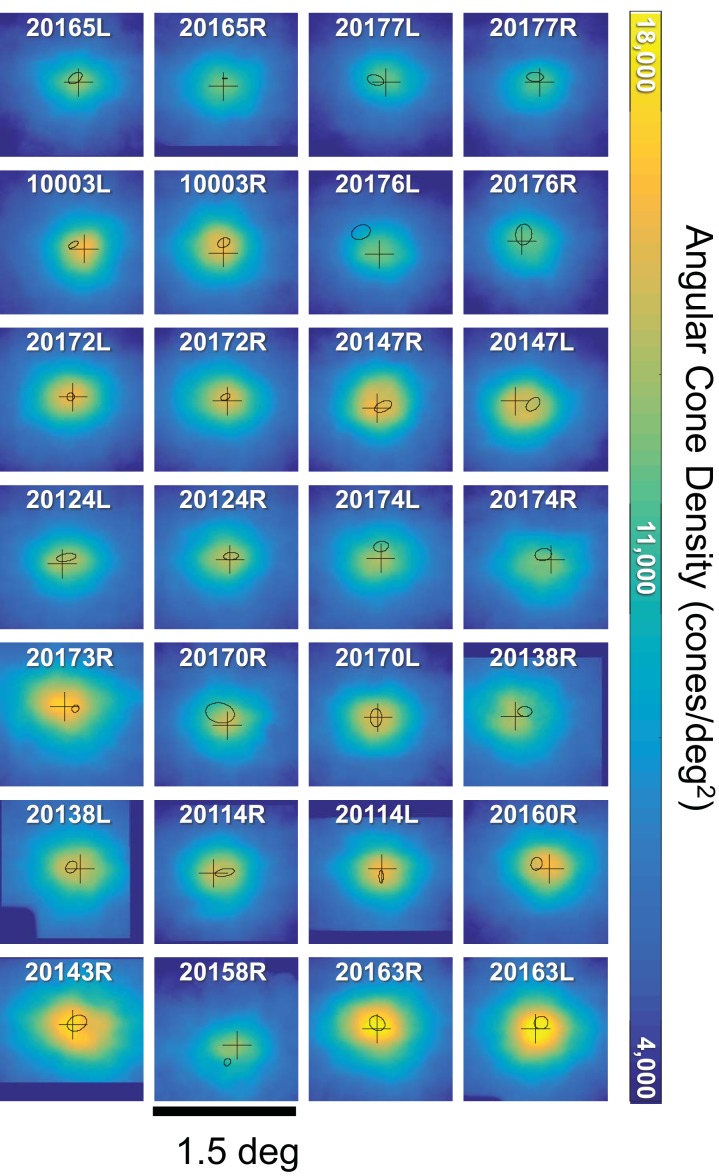
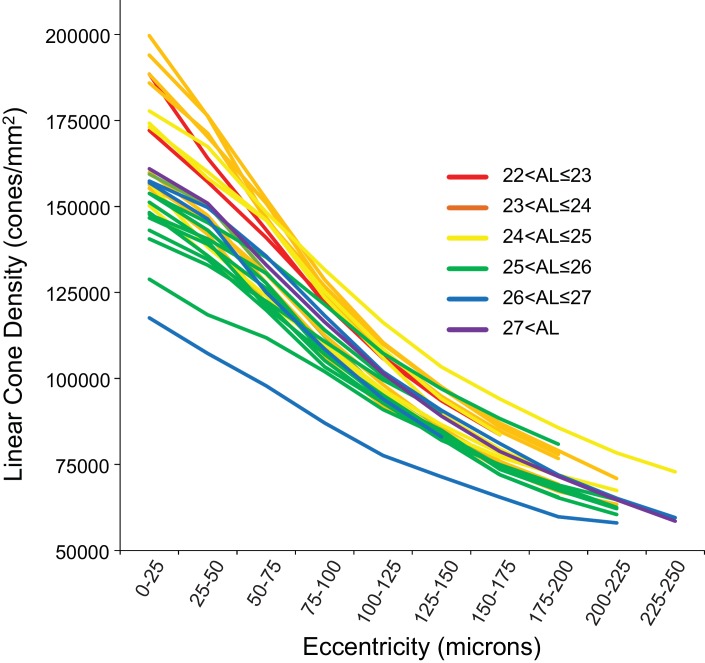
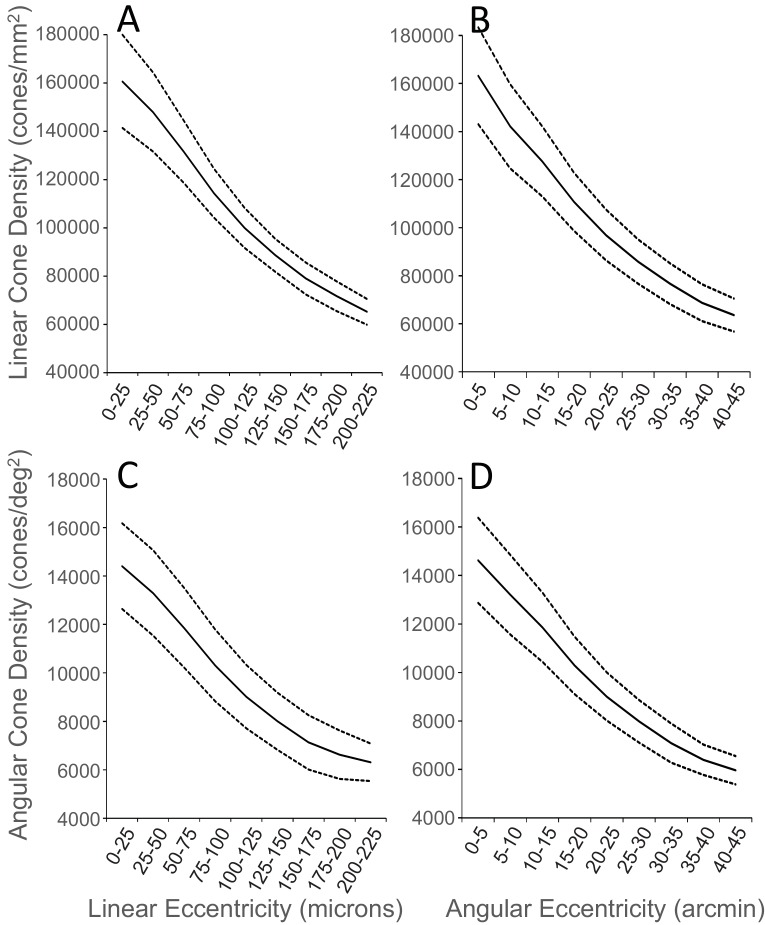
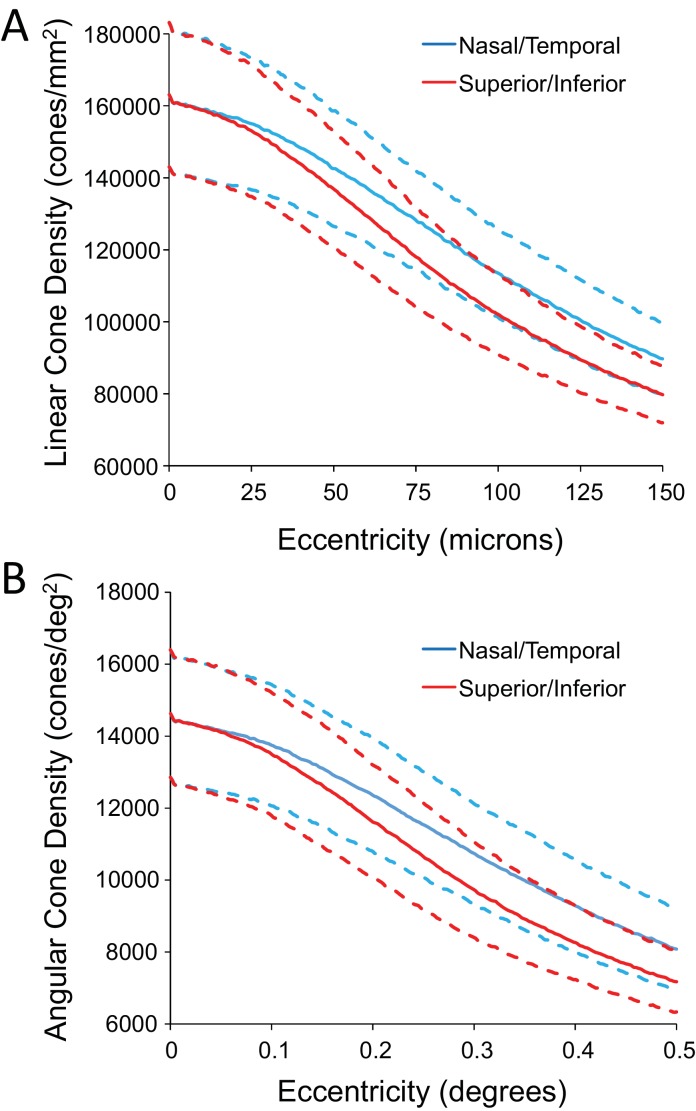
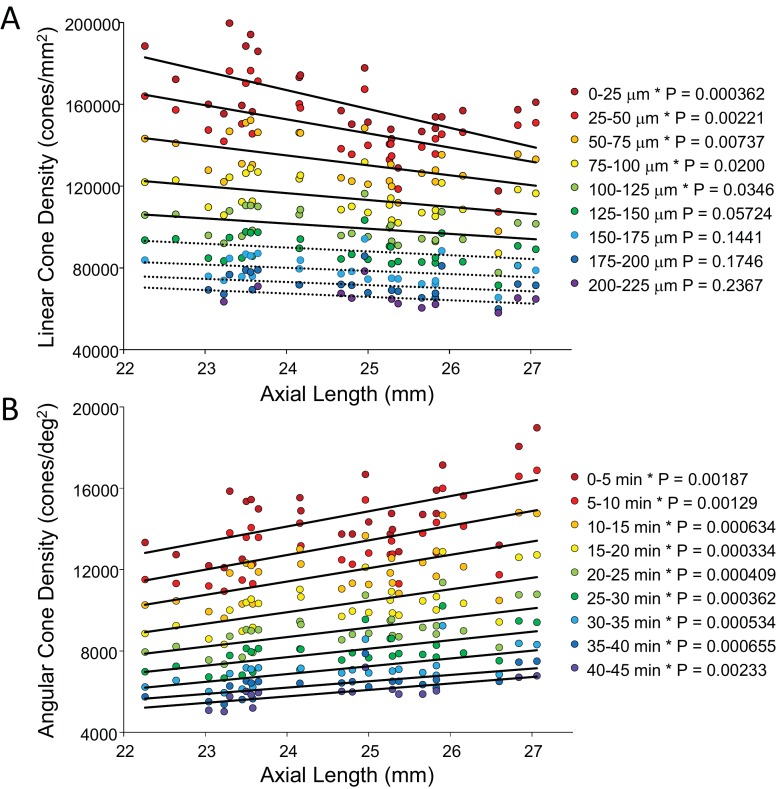
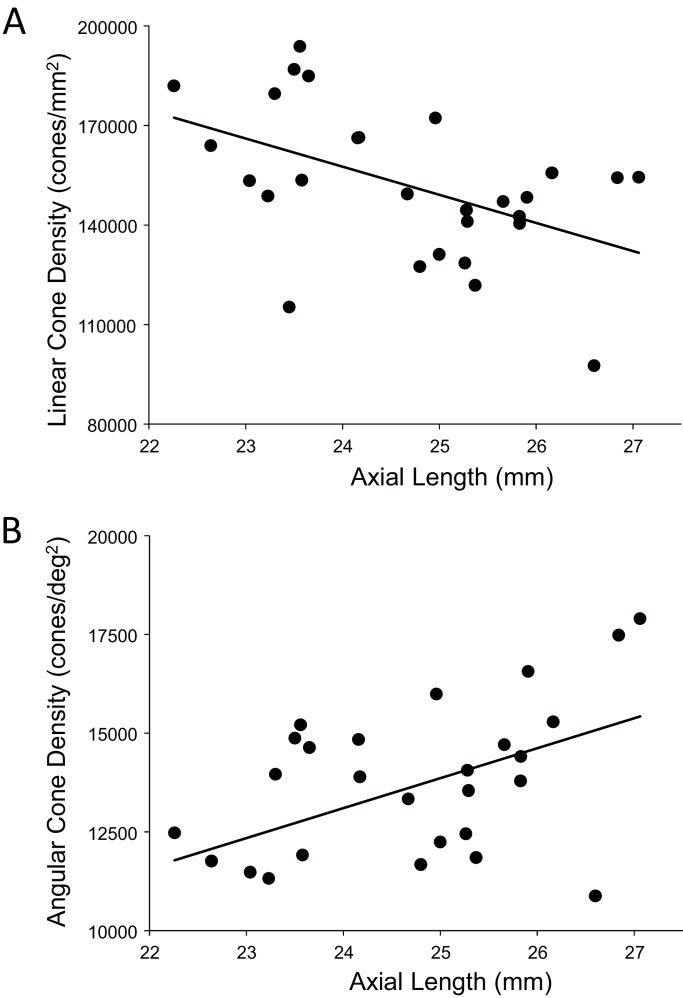
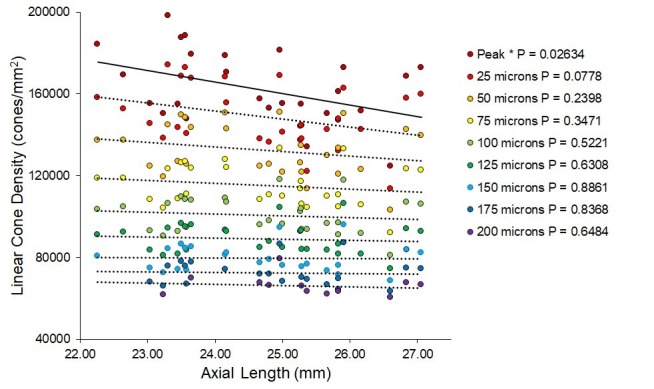
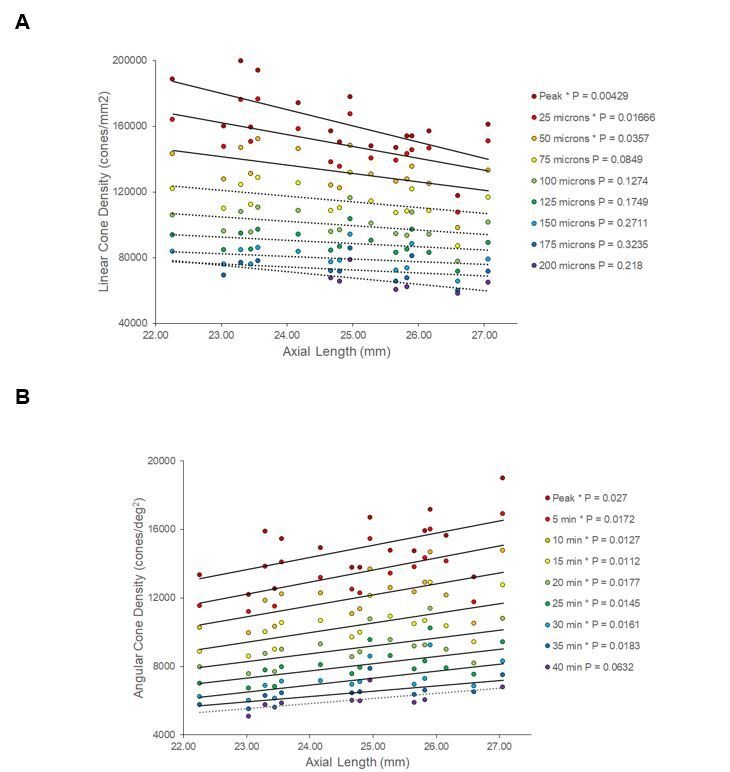
We provide the first measures of foveal cone density as a function of axial length in living eyes and discuss the physical and visual implications of our findings. We used a new generation Adaptive Optics Scanning Laser Ophthalmoscope to image cones at and near the fovea in 28 eyes of 16 subjects. Cone density and other metrics were computed in units of visual angle and linear retinal units. The foveal cone mosaic in longer eyes is expanded at the fovea, but not in proportion to eye length. Despite retinal stretching (decrease in cones/mm2), myopes generally have a higher angular sampling density (increase in cones/deg2) in and around the fovea compared to emmetropes, offering the potential for better visual acuity. Reports of deficits in best-corrected foveal vision in myopes compared to emmetropes cannot be explained by increased spacing between photoreceptors caused by retinal stretching during myopic progression.
Keywords: adaptive optics; cone photoreceptors; fovea; human; myopia; neuroscience.
© 2019, Wang et al.
Conflict of interest statement
YW, NB, PT, JM, SR No competing interests declared, AR has a patent (USPTO#7118216) assigned to the University of Houston and the University of Rochester which is currently licensed to Boston Micromachines Corp (Watertown, MA, USA). Both he and the company stand to gain financially from the publication of these results. No other authors have competing interests.
Figures
References
-
- Agaoglu M, Sit MT, Wan D, Chung ST. GitHub; 2018. https://github.com/lowvisionresearch/ReVAS
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
