

Renin-Angiotensin-Aldosterone System-based Antihypertensive Agents and the Risk of Colorectal Cancer Among Medicare Beneficiaries
- PMID: 31348009
- PMCID: PMC6768762
- DOI: 10.1097/EDE.0000000000001065
Renin-Angiotensin-Aldosterone System-based Antihypertensive Agents and the Risk of Colorectal Cancer Among Medicare Beneficiaries
Abstract
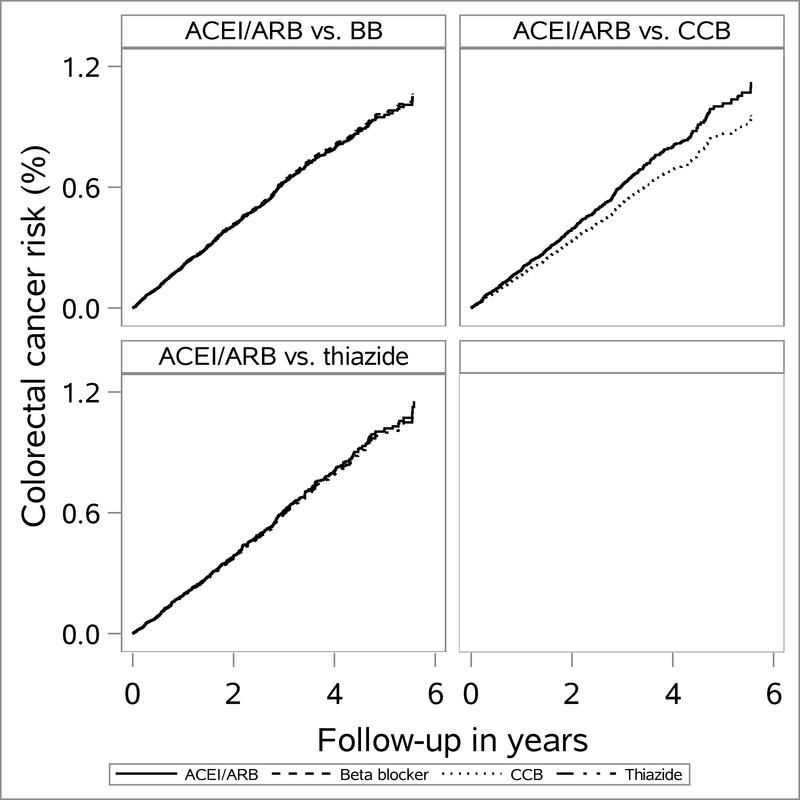
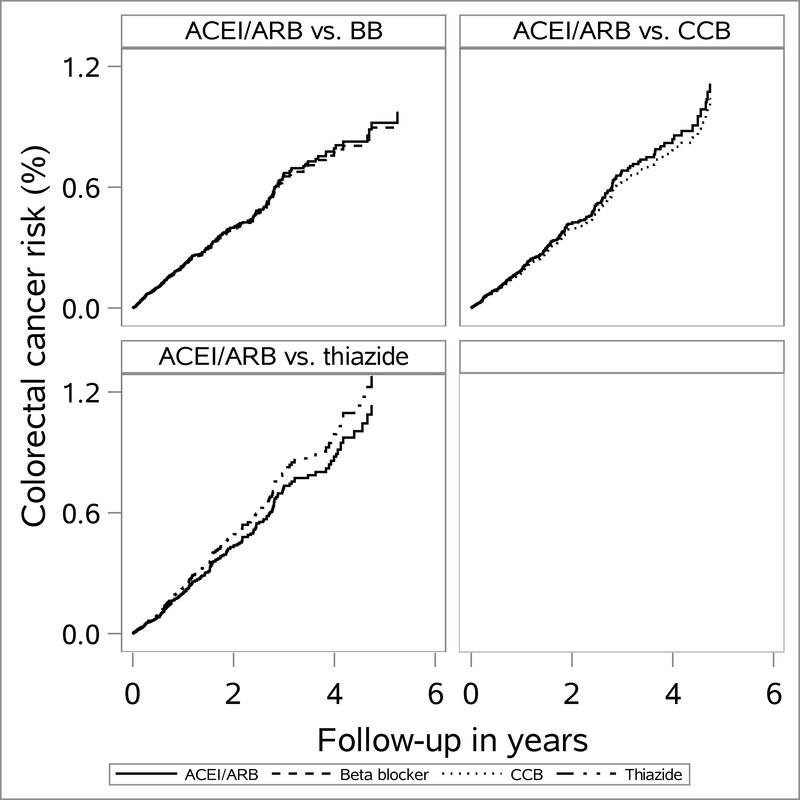
Background: Biologic evidence suggests that angiotensin II may play a role in tumor progression or growth. We compared the short-term colorectal cancer (CRC) risk among initiators of angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB) versus guideline-recommended clinical alternatives (beta blockers, calcium channel blockers [CCB], and thiazides).
Methods: We conducted a new-user cohort study on U.S. Medicare beneficiaries aged over 65 years, who initiated antihypertensive monotherapy during 2007-2013 and were free of cancer diagnosis before drug initiation. Follow-up began 6 months postinitiation to allow time for the diagnostic delay. We estimated hazard ratios (HR) with 95% confidence intervals (CI) using propensity score weighted Cox regression, overall and stratified by time since drug initiation, and 5-year cumulative risk differences (RD) using Kaplan-Meier estimator. We assessed the potential for unmeasured confounding using supplemental data from Medicare Current Beneficiary Survey.
Results: For analyses without censoring for treatment changes, we observed 532 CRC events among 111,533 ACEI/ARB initiators. After a median follow-up of 2.2 years (interquartile range: 1.0-3.7), CRC risk was similar between ACEI/ARB and active comparators, with adjusted HRs of 1.0 (95% CI = 0.85, 1.1) for ACEI/ARB versus beta blockers, 1.2 (95% CI = 0.97, 1.4) for ACEI/ARB versus CCB and 1.0 (95% CI = 0.80, 1.3) for ACEI/ARB versus thiazide. Five-year RDs and as-treated analyses, which censored follow-up at medication changes, produced similar findings.
Conclusions: Based on real-world antihypertensive utilization patterns in Medicare beneficiaries, our study suggests no association between ACEI/ARB initiation and the short-term CRC risk.
Conflict of interest statement
Conflicts of interest:
P.T.H has no conflicts of interest. T.S. reports salary support from Center for Pharmacoepidemiology in the Department of Epidemiology, Gillings School of Global Public Health (current members: GlaxoSmithKline, UCB BioSciences, Merck), research support from AstraZeneca, Amgen, and ownership interest in Novartis, Roche, BASF, AstraZeneca, Johnson & Johnson, and Novo Nordisk.
R.J.S. is a paid consultant to Amgen, Pfizer and Merck.
Figures
References
-
- Nelson DL, Lehninger AL, Cox MM. Lehninger principles of biochemistry. New York: W.H. Freeman; 2005.
-
- Fernandez LA, Twickler J, Mead A. Neovascularization produced by angiotensin II. J Lab Clin Med. 1985;105(2):141–145. - PubMed
-
- Folkman J, Watson K, Ingber D, Hanahan D. Induction of angiogenesis during the transition from hyperplasia to neoplasia. Nature. 1989;339(6219):58–61. - PubMed
-
- Daemen MJ, Lombardi DM, Bosman FT, Schwartz SM. Angiotensin II induces smooth muscle cell proliferation in the normal and injured rat arterial wall. Circ Res. 1991;68(2):450–456. - PubMed
-
- Chiu T, Santiskulvong C, Rozengurt E. ANG II stimulates PKC-dependent ERK activation, DNA synthesis, and cell division in intestinal epithelial cells. Am J Physiol Gastrointest Liver Physiol. 2003;285(1):G1–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
