

Lower limb vein thrombosis-induced pulmonary embolism and paradoxical multiple arterial embolisms: A case report with a 10-year follow-up
- PMID: 31348266
- PMCID: PMC6709194
- DOI: 10.1097/MD.0000000000016522
Lower limb vein thrombosis-induced pulmonary embolism and paradoxical multiple arterial embolisms: A case report with a 10-year follow-up
Abstract
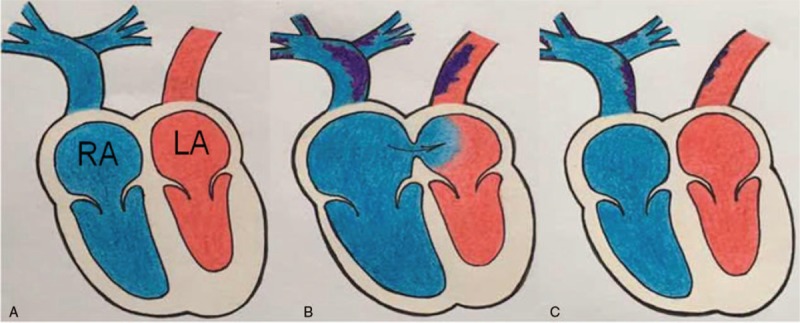
Introduction: Paradoxical embolism (PDE) refers to direct passage of venous thrombi into the arterial circulation through an arteriovenous shunt. It is well-known that the pulmonary thromboembolism (PTE) can cause opening of the foramen ovale leading to paradoxical arterial embolism. Long term follow up of PDE patient over 10 years was not reported in the literature.
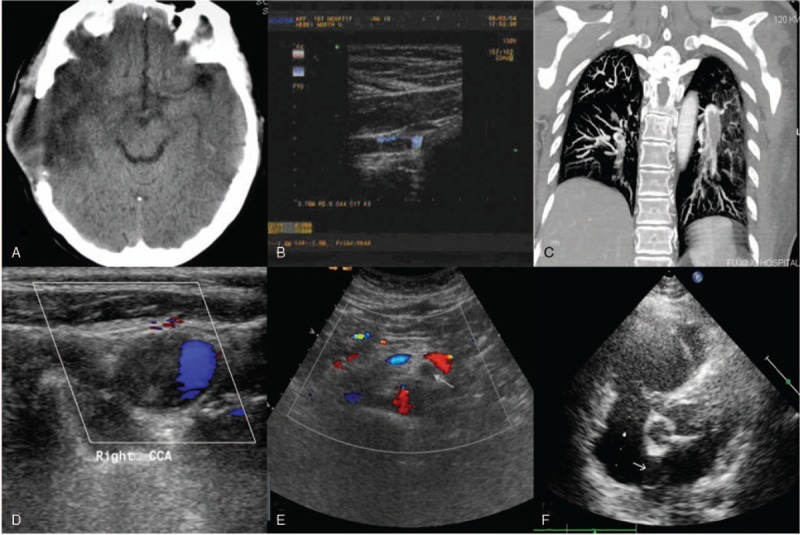
Patient concerns: A 57-year-old woman presented with initial symptoms of numbness/weakness and hypoxemia. Ultrasonography and pulmonary arteriography indicated pulmonary thromboembolism.
Diagnosis: Pulmonary embolism and paradoxical multiple arterial embolism or acute PTE concomitant with paradoxical multiple arterial embolism.
Interventions: Craniectomy and anticoagulation treatment was administered and the patient received low-dose warfarin therapy for 10 years.
Outcomes: The patient is currently stable with no abnormalities seen in the deep veins of the bilateral lower limbs. The international normalized ratio (INR) was controlled within the range of 1.20 to 1.51. As this is a 10-year follow-up case report, the patient has responded well to the treatment and has been followed-up. The follow-up has been annual and the patient has been stable CONCLUSION:: Low intensity and persistent anticoagulation therapy can inhibit blood thrombophilia and reduce the risk of bleeding. It is noteworthy that such an approach used effectively in this patient. To best our knowledge, it is first report for long term follow up PDE patient successfully over 10 years.
Conflict of interest statement
The authors declare that there are no conflicts of interest in this work.
Figures
References
-
- Mustafa FE, Bilge Ö, Aylin O, et al. The relationship of patent foramen ovale location with severity of stroke: a new risk factor for paradoxical embolism. Acta Clin Belg 2016;71:149–53. - PubMed
-
- Windecker S, Stortecky S, Meier B. Paradoxical Embolism. J Am Coll Cardiol 2014;64:403–15. - PubMed
-
- Abad-Arranz M, Jara-Palomares L, Martos-Maine JL, et al. Embolism and concomitant paradoxical embolism. a case report. Arch Bronconeumol 2014;50:120–2. - PubMed
-
- Tang CE. Paradoxical embolism: a rare life- and limb-threatening emergency. Can J Emerg Med 2004;6:40–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
