

Teaching simulated arthroscopic Bankart repair: residents’ assessment at the Annual Shoulder Course
- PMID: 31348628
- PMCID: PMC6660270
- DOI: 10.1503/cjs.004618
Teaching simulated arthroscopic Bankart repair: residents’ assessment at the Annual Shoulder Course
Abstract
Background: This study’s aim was to evaluate the performance of senior orthopedic residents during simulated arthroscopic anterior stabilization (Bankart repair) before and after a national shoulder review course.
Methods: Participants were assessed before and after the Annual Shoulder Review Course over a 3-day period, using a multiple-choice examination and surgery performance assessment. The surgical evaluation was completed by fellowship-trained surgeons using a standardized procedure checklist and a global rating scale. All Canadian senior orthopedic residents were invited to participate in the course.
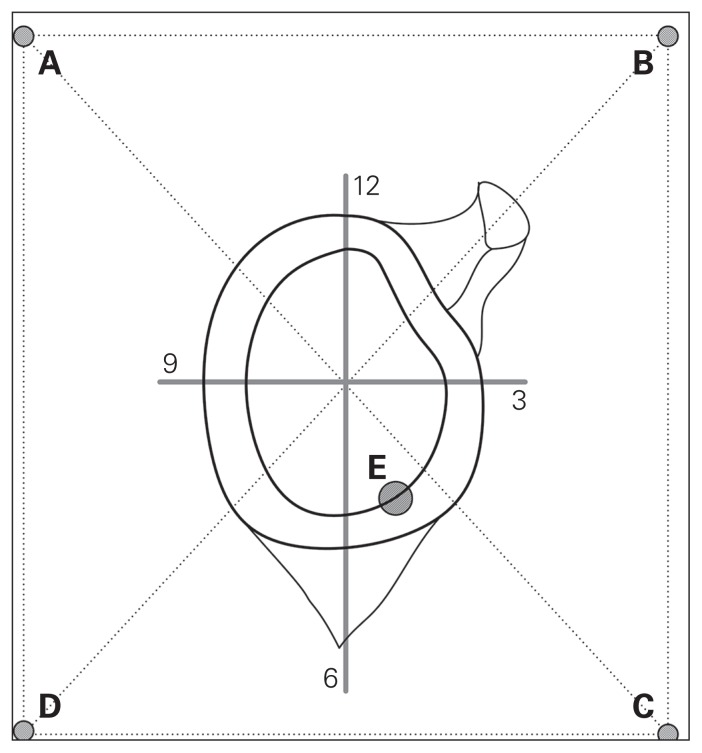
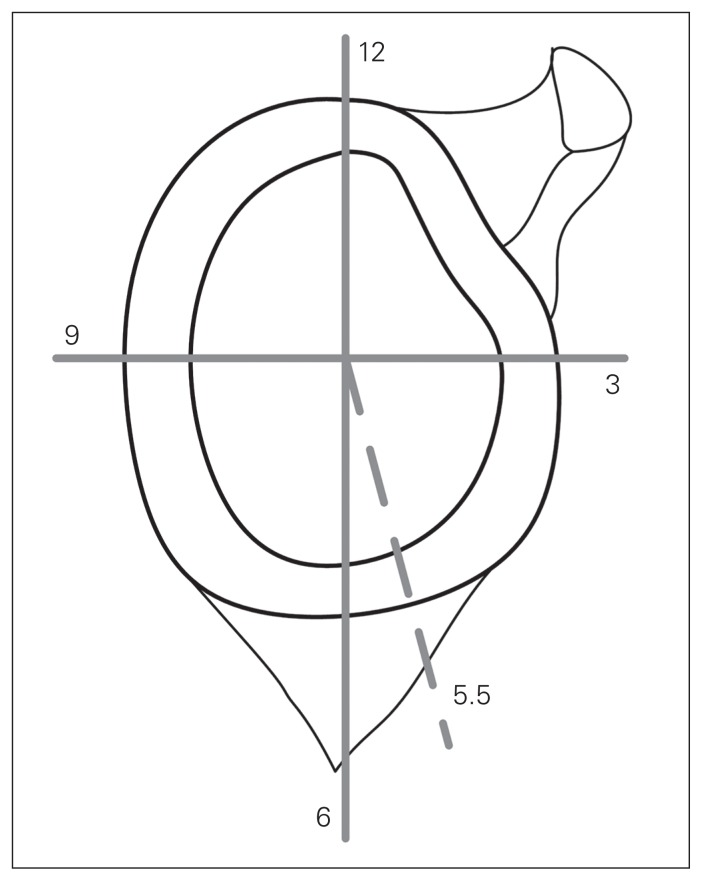
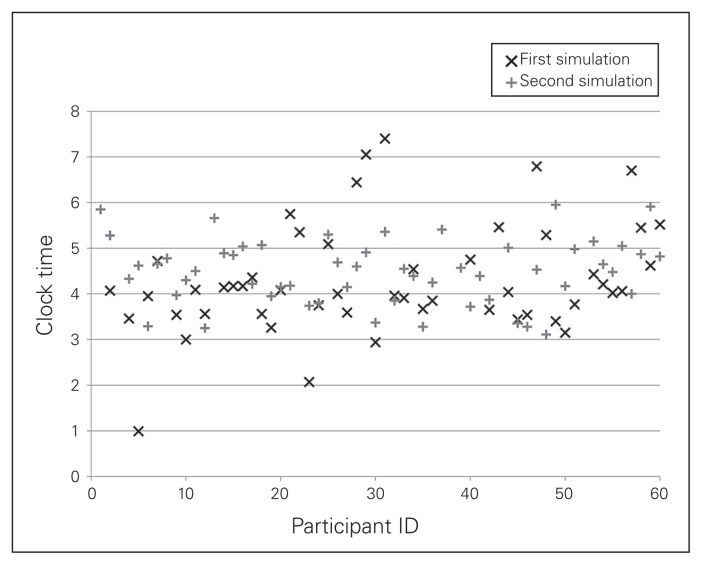
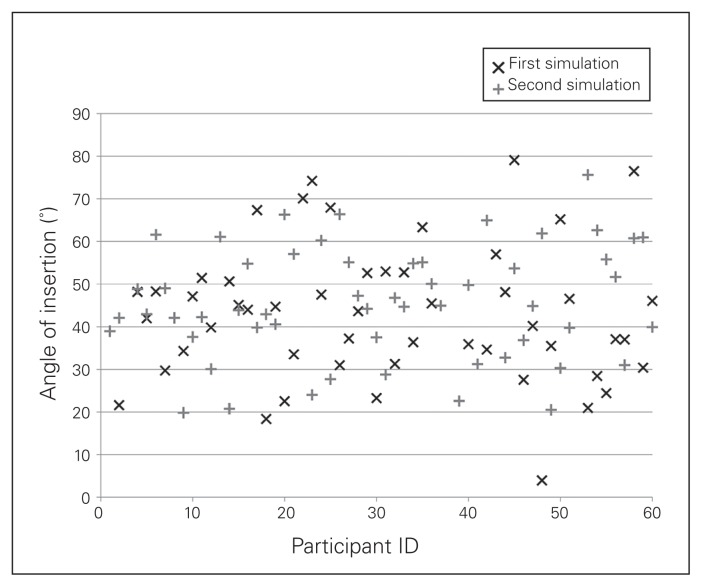
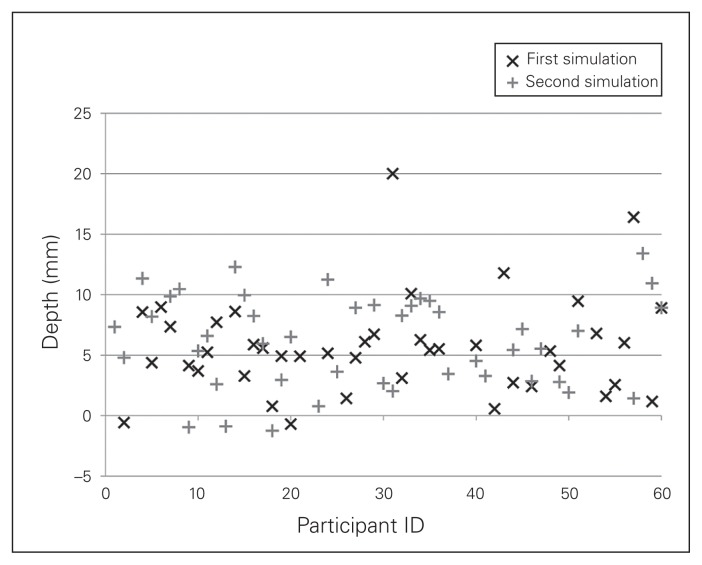
Results: The 57 participants showed improvement following the course. The written knowledge evaluation mean score increased, and all 3 surgical performance measurements improved: surgical task time improved from 4:40 min to 2:53 min (p < 0.001), surgical technique evaluation increased from 56% to 67% after the procedure checklist (p < 0.001), and anchor placement improved for all 3 aspects. Anchor entry point was the sole measure not to improve enough to reach statistical significance (p = 0.37).
Conclusion: Our data support the inclusion of dry model surgical simulation as part of a surgical skills course for both training and assessment of orthopedic surgery residents.
Contexte: Le but de cette étude était d’évaluer le rendement des résidents seniors en orthopédie durant une simulation de stabilisation arthroscopique antérieure (intervention de Bankart) avant et après un cours de révision national sur l’articulation de l’épaule.
Méthodes: Les participants ont été évalués avant et après l’Annual Shoulder Review Course sur une période de 3 jours, à l’aide d’un examen à choix multiples et d’une épreuve chirurgicale pratique. L’évaluation chirurgicale était effectuée par des chirurgiens spécialisés, à l’aide d’une liste de vérification normalisée des procédures et d’une échelle d’évaluation globale. Tous les résidents séniors canadiens en orthopédie étaient invités à participer au cours.
Résultats: Les 57 participants ont montré une amélioration après le cours. Lesrésultats à l’examen écrit ont augmenté, tout comme ceux des 3 évaluations chirurgicales : le temps chirurgical a diminué, passant de 4:40 min à 2:53 min (p < 0,001), l’évaluation de la technique chirurgicale a augmenté de 56 % à 67 % selon la liste de vérification (p < 0,001) et le positionnement des ancres s’est aussi amélioré pour les 3 positionnements. Le point d’entrée des ancres a été la seule mesure à ne pas s’améliorer suffisamment pour atteindre une portée statistique (p = 0,37).
Conclusion: Nos données appuient l’inclusion d’un modèle de simulation sec pour la formation et l’évaluation des résidents en chirurgie orthopédique.
© 2019 Joule Inc. or its licensors
Conflict of interest statement
D. Rouleau is a consultant for Bioventus and Wright Medical. V. Godbout has received speaker fees from Arthrex.
Figures
References
-
- Fitts PM, Posner MI. Human performance. Belmont (CA): Brooks/Cole; 1967.
-
- Hamdorf JM, Hall JC. Acquiring surgical skills. Br J Surg. 2000;87:28–37. - PubMed
-
- Pedowitz R, Marsh L. Motor skills training in orthopaedic surgery: a paradigm shift toward a simulation-based educational curriculum. J Am Acad Orthop Surg. 2012;20:407–9. - PubMed
-
- Zendejas B, Brydges R, Hamstra SJ, et al. State of the evidence on simulation-based training for laparoscopic surgery, a systematic review. Ann Surg. 2013;257:586–93. - PubMed
-
- Kneebone RL, Scott W, Darzi A, et al. Simulation and clinical practice: strengthening the relationship. Med Educ. 2004;38:1095–102. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical