

Malnutrition, nutritional interventions and clinical outcomes of patients with acute small bowel obstruction: results from a national, multicentre, prospective audit
- PMID: 31352419
- PMCID: PMC6661661
- DOI: 10.1136/bmjopen-2019-029235
Malnutrition, nutritional interventions and clinical outcomes of patients with acute small bowel obstruction: results from a national, multicentre, prospective audit
Abstract
Objective: The aim of this study was to assess the nutritional status of patients presenting with small bowel obstruction (SBO), along with associated nutritional interventions and clinical outcomes.
Design: Prospective cohort study.
Setting: 131 UK hospitals with acute surgical services.
Participants: 2069 adult patients with a diagnosis of SBO were included in this study. The mean age was 67.0 years and 54.7% were female.
Primary and secondary outcome measures: Primary outcome was in-hospital mortality. Secondary outcomes recorded included: major complications (composite of in-hospital mortality, reoperation, unplanned intensive care admission and 30-day readmission), complications arising from surgery (anastomotic leak, wound dehiscence), infection (pneumonia, surgical site infection, intra-abdominal infection, urinary tract infection, venous catheter infection), cardiac complications, venous thromboembolism and delirium.
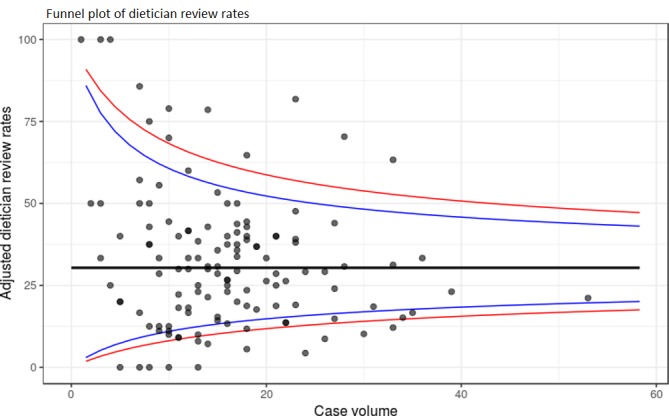
Results: Postoperative adhesions were the most common cause of SBO (49.1%). Early surgery (<24 hours postadmission) took place in 30.0% of patients, 22.0% underwent delayed operation and 47.9% were managed non-operatively. Malnutrition as stratified by Nutritional Risk Index was common, with 35.7% at moderate risk and 5.7% at severe risk of malnutrition. Dietitian review occurred in just 36.4% and 55.9% of the moderate and severe risk groups. In the low risk group, 30.3% received nutritional intervention compared with 40.7% in moderate risk group and 62.7% in severe risk group. In comparison to the low risk group, patients who were at severe or moderate risk of malnutrition had 4.2 and 2.4 times higher unadjusted risk of in-hospital mortality, respectively. Propensity-matched analysis found no difference in outcomes based on use or timing of parenteral nutrition.
Conclusions: Malnutrition on admission is associated with worse outcomes in patients with SBO, and marked variation in management of malnutrition was observed. Future trials should focus on identifying effective and cost-effective nutritional interventions in SBO.
Keywords: adult surgery; nutritional support; perioperative care.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures






References
-
- National Emergency Laparotomy Audit. Third Report of the National Emergency Laparotomy Audit. London: Royal College of Anaesthetists, 2018.
-
- Jafari MD, Jafari F, Foe-Paker JE, et al. Adhesive small bowel obstruction in the united states: Has laparoscopy made an impact? Am Surg 2015;81:1028–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical