

White Matter in Schizophrenia Treatment Resistance
- PMID: 31352812
- PMCID: PMC6773514
- DOI: 10.1176/appi.ajp.2019.18101212
White Matter in Schizophrenia Treatment Resistance
Abstract
Objective: Failure of antipsychotic medications to resolve symptoms in patients with schizophrenia creates a clinical challenge that is known as treatment resistance. The causes of treatment resistance are unknown, but it is associated with earlier age at onset and more severe cognitive deficits. The authors tested the hypothesis that white matter deficits that are involved in both neurodevelopment and severity of cognitive deficits in schizophrenia are associated with a higher risk of treatment resistance.
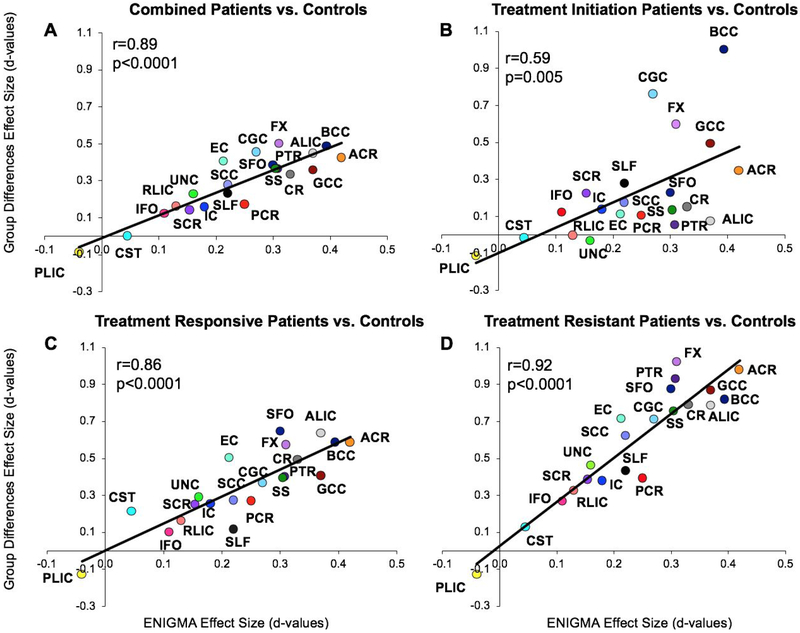
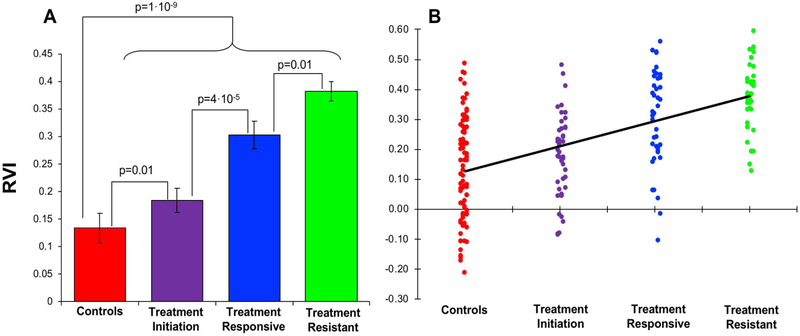
Methods: The study sample (N=122; mean age, 38.2 years) included schizophrenia patients at treatment initiation (N=45), patients whose symptoms were treatment responsive (N=40), and patients whose symptoms were treatment resistant (N=37), as well as healthy control subjects (N=78; mean age, 39.2 years). White matter regional vulnerability index (RVI) was tested as a predictor of treatment resistance and cognitive deficits. Higher RVI is indicative of better agreement between diffusion tensor imaging fractional anisotropy across the brain in an individual and the pattern identified by the largest-to-date meta-analysis of white matter deficits in schizophrenia.
Results: Patients with treatment-resistant symptoms showed the highest white matter RVI (mean=0.38 [SD=0.2]), which was significantly higher than the RVI among patients with treatment-responsive symptoms (mean=0.30 [SD=0.02]). At the onset of treatment, schizophrenia patients showed significantly higher RVI than healthy control subjects (mean=0.18 [SD=0.03] and mean=0.13 [SD=0.02], respectively). RVIs were significantly correlated with performance on processing speed and negative symptoms.
Conclusions: Schizophrenia affects white matter microstructure in specific regional patterns. Susceptibility to white matter regional deficits is associated with an increased likelihood of treatment resistance. Developments to overcome schizophrenia treatment resistance should consider white matter as an important target.
Keywords: Magnetic Resonance Imaging; Schizophrenia.
Conflict of interest statement
Conflict of Interest
LEH has received or plans to receive research funding or consulting fees on research projects from Mitsubishi, Your Energy Systems LLC, Neuralstem, Taisho, Heptares, Pfizer, Sound Pharma, Takeda, and Regeneron. None was involved in the design, analysis or outcomes of the study. PT and NJ have received research funding, unrelated to this work, from Biogen. All other authors declare no conflicts of interest.
Figures

References
-
- Howes OD, McCutcheon R, Agid O, de Bartolomeis A, van Beveren NJ, Birnbaum ML, Bloomfield MA, Bressan RA, Buchanan RW, Carpenter WT, Castle DJ, Citrome L, Daskalakis ZJ, Davidson M, Drake RJ, Dursun S, Ebdrup BH, Elkis H, Falkai P, Fleischacker WW, Gadelha A, Gaughran F, Glenthoj BY, Graff-Guerrero A, Hallak JE, Honer WG, Kennedy J, Kinon BJ, Lawrie SM, Lee J, Leweke FM, MacCabe JH, McNabb CB, Meltzer H, Moller HJ, Nakajima S, Pantelis C, Reis Marques T, Remington G, Rossell SL, Russell BR, Siu CO, Suzuki T, Sommer IE, Taylor D, Thomas N, Ucok A, Umbricht D, Walters JT, Kane J, Correll CU. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology. Am J Psychiatry. 2017;174:216–229. - PMC - PubMed
-
- Samara MT, Dold M, Gianatsi M, Nikolakopoulou A, Helfer B, Salanti G, Leucht S. Efficacy, Acceptability, and Tolerability of Antipsychotics in Treatment-Resistant Schizophrenia: A Network Meta-analysis. JAMA Psychiatry. 2016;73:199–210. - PubMed
-
- Kulkarni J, Gavrilidis E, Wang W, Worsley R, Fitzgerald PB, Gurvich C, Van Rheenen T, Berk M, Burger H. Estradiol for treatment-resistant schizophrenia: a large-scale randomized-controlled trial in women of child-bearing age. Mol Psychiatry. 2015;20:695–702. - PubMed
-
- Hoffman RE, Hawkins KA, Gueorguieva R, Boutros NN, Rachid F, Carroll K, Krystal JH. Transcranial magnetic stimulation of left temporoparietal cortex and medication-resistant auditory hallucinations. Arch Gen Psychiatry. 2003;60:49–56. - PubMed
-
- Heresco-Levy U, Ermilov M, Shimoni J, Shapira B, Silipo G, Javitt DC. Placebo-controlled trial of D-cycloserine added to conventional neuroleptics, olanzapine, or risperidone in schizophrenia. Am J Psychiatry. 2002;159:480–482. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
