

Efficacy and safety of total glucosides of paeony combined with methotrexate and leflunomide for active rheumatoid arthritis: a meta-analysis
- PMID: 31354242
- PMCID: PMC6588713
- DOI: 10.2147/DDDT.S207226
Efficacy and safety of total glucosides of paeony combined with methotrexate and leflunomide for active rheumatoid arthritis: a meta-analysis
Abstract
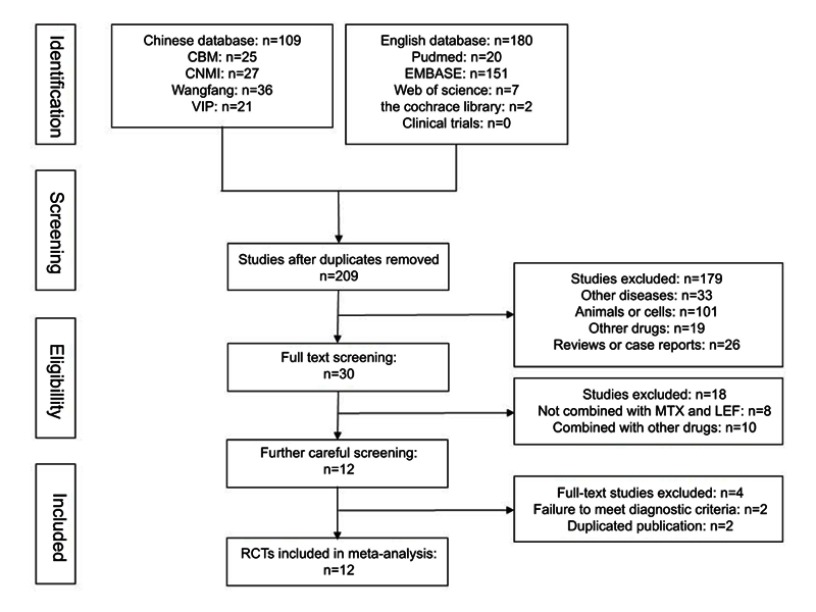
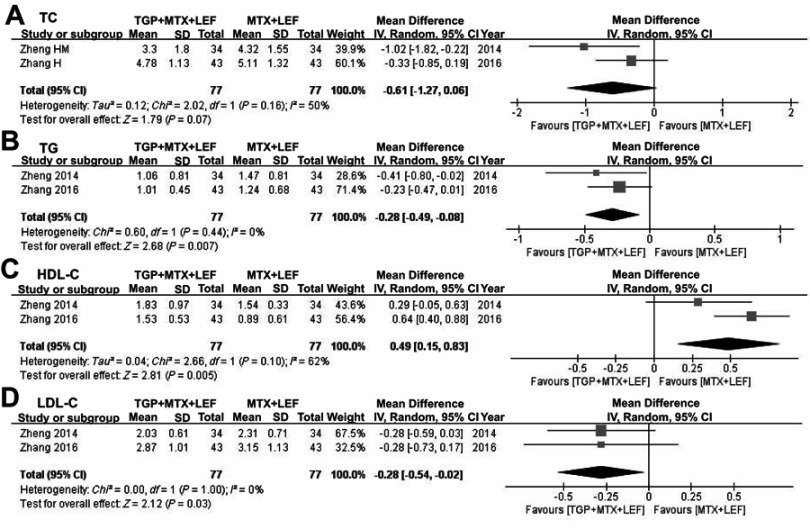
Purpose: Total glucosides of paeony (TGP) have been confirmed to reduce hepatotoxicity caused by methotrexate (MTX) and leflunomide (LEF) in rheumatoid arthritis (RA). Nevertheless, high-quality evidence-based meta-analysis data on the issue are unavailable. This study aimed to evaluate the efficacy and safety of this combination treatment for RA. Materials and methods: PubMed, EMBASE, Web of Science, Cochrane Library, ClinicalTrials, Chinese Biomedical Literature database, China National Knowledge Internet, Wan Fang, and VIP were searched up to February 2019. Randomized controlled trials (RCTs) on the efficacy and safety of TGP combined MTX and LEF for RA were included. Results: Eight RCTs were included in the final meta-analysis. Pooled results showed better therapeutic effects against RA in the TGP-treated group (RR =1.10, 95% CI: 1.04 -1.16). The TGP+MTX+LEF group showed a reduced erythrocyte sedimentation rate (MD = -2.80 mm/h, 95% CI: -5.08 - -0.52), C-reactive protein level (MD = -4.17 mg/L, 95% CI: -7.84 - -0.51), and rheumatoid factor (MD = -12.09 IU/mL, 95% CI: -14.05 - -10.14). Besides, the combination treatment tended to benefit lipid profiles (total cholesterol: 95% CI: -1.27-0.06; triglycerides: 95% CI: -0.49 - -0.08; high-density lipoprotein cholesterol: 95% CI: 0.15-0.83; and low-density lipoprotein cholesterol: 95% CI: -0.54 - -0.02). Adverse events, hepatotoxicity in particular, significantly decreased (RR =0.55, 95% CI: 0.38-0.80) in the TGP group. Conclusion: Compared to MTX and LEF therapy, TGP combination treatment may be a more effective and safer strategy. It is advisable to apply TGP as an adjuvant given its hepatoprotective and possible lipid-regulating effect. However, further large-scale and high-quality clinical trials are warranted, and the efficacy of TGP in terms of its effect on lipid profiles should be further confirmed.
Keywords: leflunomide; meta-analysis; methotrexate; rheumatoid arthritis; total glucosides of paeony.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures






References
-
- Katchamart W, Trudeau J, Phumethum V, Bombardier C. Efficacy and toxicity of methotrexate (MTX) monotherapy versus MTX combination therapy with non-biological disease-modifying antirheumatic drugs in rheumatoid arthritis: a systematic review and meta-analysis. Ann Rheum Dis. 2009;68(7):1105–1112. doi:10.1136/ard.2008.099861 - DOI - PMC - PubMed
-
- Nam JL, Takase-Minegishi K, Ramiro S, et al. Efficacy of biological disease-modifying antirheumatic drugs: a systematic literature review informing the 2016 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis. 2017;76(6):1113–1136. doi:10.1136/annrheumdis-2016-210713 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
