

Prevention of postoperative delirium in elderly patients planned for elective surgery: systematic review and meta-analysis
- PMID: 31354253
- PMCID: PMC6590846
- DOI: 10.2147/CIA.S201323
Prevention of postoperative delirium in elderly patients planned for elective surgery: systematic review and meta-analysis
Abstract
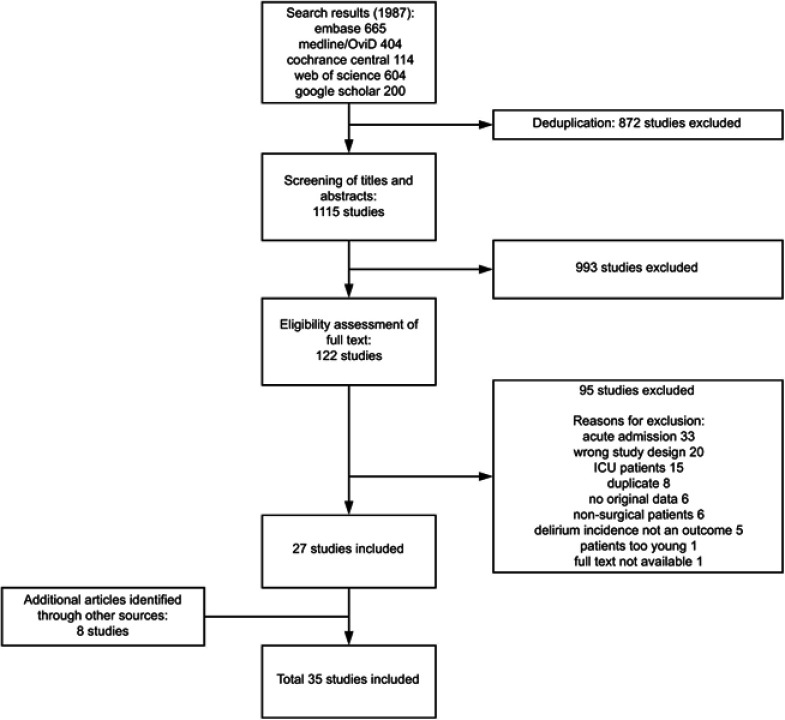
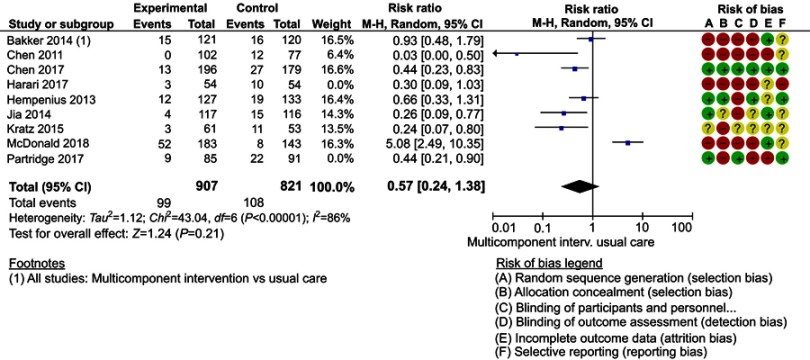
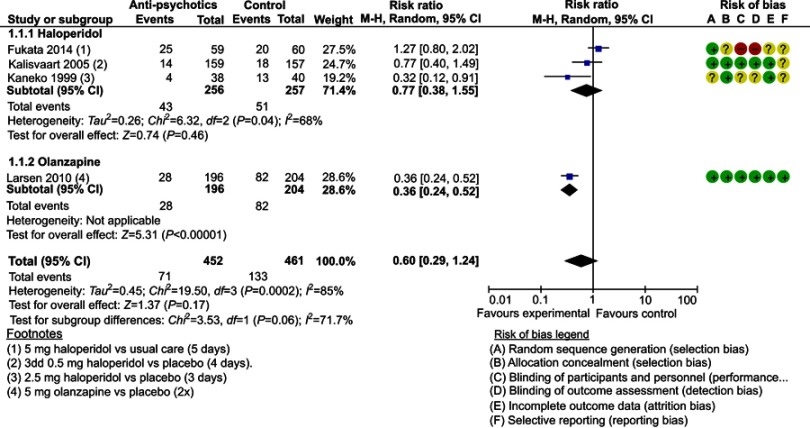
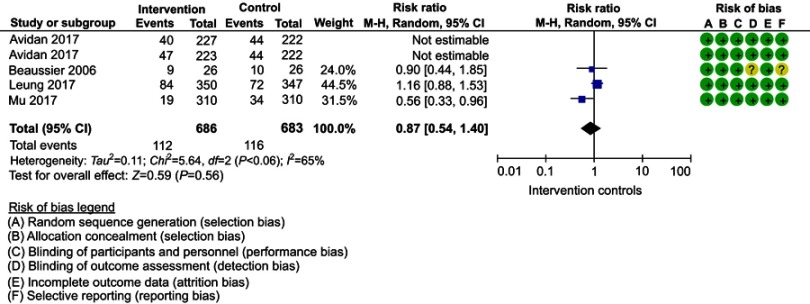
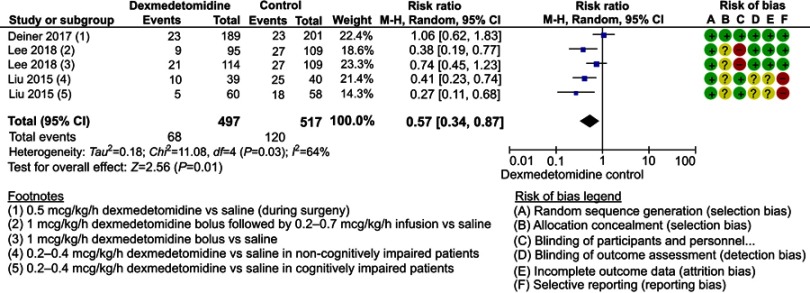
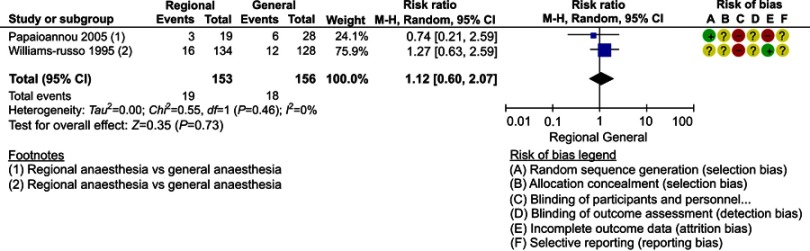
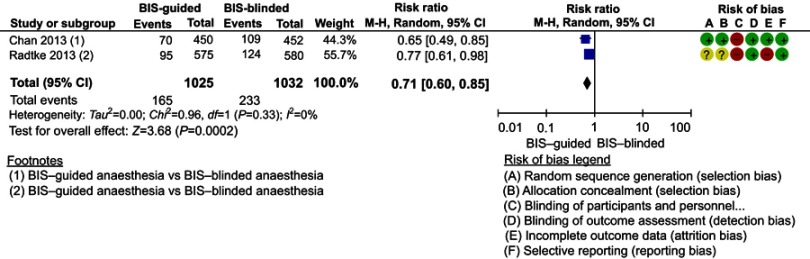
Introduction: Vulnerable or "frail" patients are susceptible to the development of delirium when exposed to triggers such as surgical procedures. Once delirium occurs, interventions have little effect on severity or duration, emphasizing the importance of primary prevention. This review provides an overview of interventions to prevent postoperative delirium in elderly patients undergoing elective surgery. Methods: A literature search was conducted in March 2018. Randomized controlled trials (RCTs) and before-and-after studies on interventions with potential effects on postoperative delirium in elderly surgical patients were included. Acute admission, planned ICU admission, and cardiac patients were excluded. Full texts were reviewed, and quality was assessed by two independent reviewers. Primary outcome was the incidence of delirium. Secondary outcomes were severity and duration of delirium. Pooled risk ratios (RRs) were calculated for incidences of delirium where similar intervention techniques were used. Results: Thirty-one RCTs and four before-and-after studies were included for analysis. In 19 studies, intervention decreased the incidences of postoperative delirium. Severity was reduced in three out of nine studies which reported severity of delirium. Duration was reduced in three out of six studies. Pooled analysis showed a significant reduction in delirium incidence for dexmedetomidine treatment, and bispectral index (BIS)-guided anaesthesia. Based on sensitivity analyses, by leaving out studies with a high risk of bias, multicomponent interventions and antipsychotics can also significantly reduce the incidence of delirium. Conclusion: Multicomponent interventions, the use of antipsychotics, BIS-guidance, and dexmedetomidine treatment can successfully reduce the incidence of postoperative delirium in elderly patients undergoing elective, non-cardiac surgery. However, present studies are heterogeneous, and high-quality studies are scarce. Future studies should add these preventive methods to already existing multimodal and multidisciplinary interventions to tackle as many precipitating factors as possible, starting in the pre-admission period.
Keywords: elderly; elective surgery; postoperative delirium; prevention.
Conflict of interest statement
The Ph.D. program of the corresponding author (T.L. Janssen) is funded by an “unrestricted grant” by Amphia Fund for innovation. The authors report no other conflicts of interest in this work.
Figures


Similar articles
-
Multimodal prehabilitation to reduce the incidence of delirium and other adverse events in elderly patients undergoing elective major abdominal surgery: An uncontrolled before-and-after study.PLoS One. 2019 Jun 13;14(6):e0218152. doi: 10.1371/journal.pone.0218152. eCollection 2019. PLoS One. 2019. PMID: 31194798 Free PMC article.
-
Pharmacologic prevention of postoperative delirium after on-pump cardiac surgery: A meta-analysis of randomized trials.Medicine (Baltimore). 2018 Oct;97(43):e12771. doi: 10.1097/MD.0000000000012771. Medicine (Baltimore). 2018. PMID: 30412068 Free PMC article. Review.
-
Postoperative delirium in elderly after elective and acute colorectal surgery: A prospective cohort study.Int J Surg. 2015 Jun;18:216-9. doi: 10.1016/j.ijsu.2015.04.080. Epub 2015 Apr 30. Int J Surg. 2015. PMID: 25937152
-
Patient safety, cost-effectiveness, and quality of life: reduction of delirium risk and postoperative cognitive dysfunction after elective procedures in older adults-study protocol for a stepped-wedge cluster randomized trial (PAWEL Study).Trials. 2019 Jan 21;20(1):71. doi: 10.1186/s13063-018-3148-8. Trials. 2019. PMID: 30665435 Free PMC article.
-
Identifying Older Adults at Risk of Delirium Following Elective Surgery: A Systematic Review and Meta-Analysis.J Gen Intern Med. 2018 Apr;33(4):500-509. doi: 10.1007/s11606-017-4204-x. Epub 2018 Jan 26. J Gen Intern Med. 2018. PMID: 29374358 Free PMC article.
Cited by
-
Association between frailty and postoperative delirium: a meta-analysis of cohort study.Aging Clin Exp Res. 2022 Jan;34(1):25-37. doi: 10.1007/s40520-021-01828-9. Epub 2021 Apr 8. Aging Clin Exp Res. 2022. PMID: 33834367
-
Bibliometric Analysis of the Top-100 Cited Articles on Postoperative Delirium.J Multidiscip Healthc. 2024 Jun 22;17:2961-2972. doi: 10.2147/JMDH.S465947. eCollection 2024. J Multidiscip Healthc. 2024. PMID: 38933695 Free PMC article.
-
The Impact of Blood Transfusion in Developing Postoperative Delirium in Patients with Hip Fracture Surgery.J Clin Med. 2023 Jul 14;12(14):4696. doi: 10.3390/jcm12144696. J Clin Med. 2023. PMID: 37510810 Free PMC article.
-
Delirium in the intensive care unit and its importance in the post-operative context: A review.Front Med (Lausanne). 2023 Mar 30;10:1071854. doi: 10.3389/fmed.2023.1071854. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37064025 Free PMC article. Review.
-
Effectiveness of a Multi-component Delirium Prevention Program Implemented on General Medicine Hospital Units: an Interrupted Time Series Analysis.J Gen Intern Med. 2023 Oct;38(13):2936-2944. doi: 10.1007/s11606-023-08238-9. Epub 2023 Jul 10. J Gen Intern Med. 2023. PMID: 37429974 Free PMC article.
References
-
- Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
