

Peripherally Embolizing Aortic Thrombus: The Work-Up, Management, and Outcome of Primary Aortic Thrombus
- PMID: 31355013
- PMCID: PMC6636506
- DOI: 10.1155/2019/8132578
Peripherally Embolizing Aortic Thrombus: The Work-Up, Management, and Outcome of Primary Aortic Thrombus
Abstract
Background: Primary aortic thrombus is an uncommon entity and not frequently reported in the literature. Herein, we discuss the presentation and management of a patient with a primary thoracic mural thrombus.
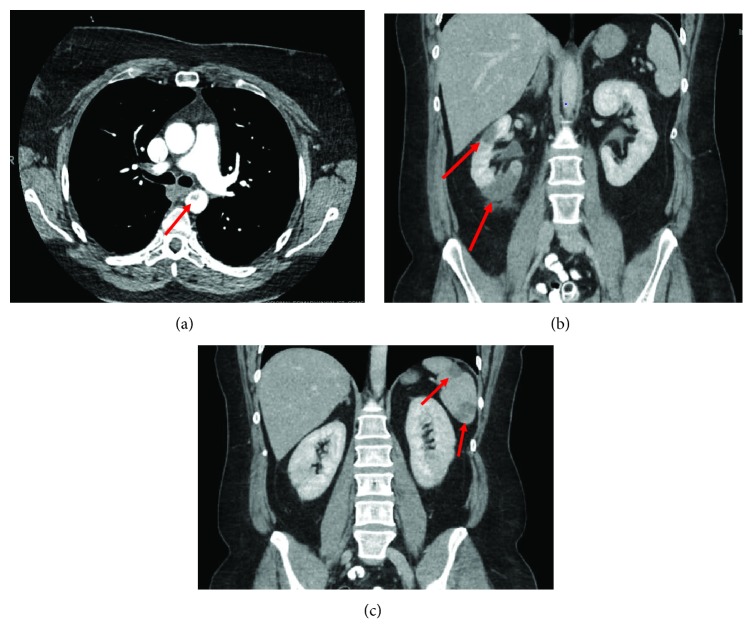
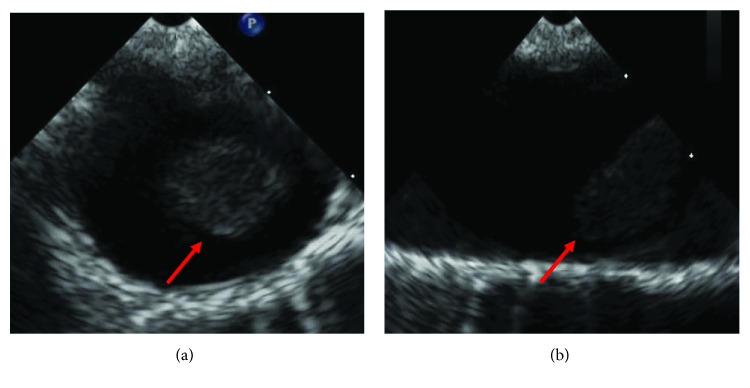
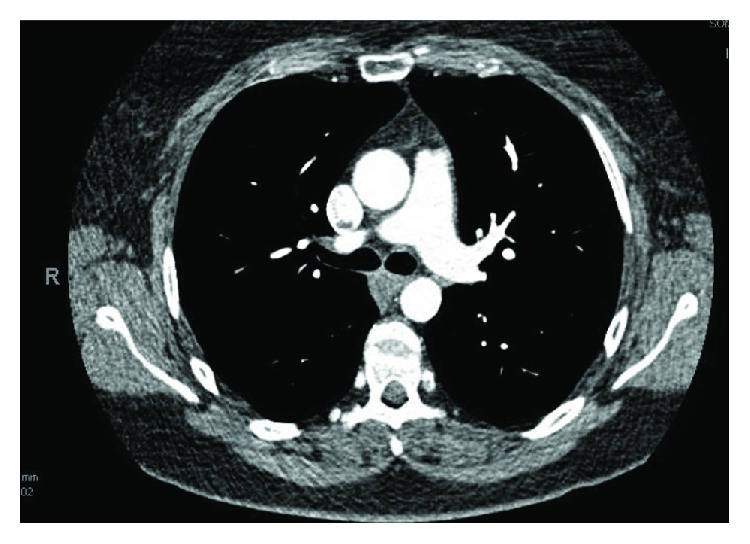
Case summary: A 46-year-old female with past medical history of tobacco dependence presented for low-grade fever and sudden onset, severe right upper quadrant abdominal pain with associated nausea and vomiting. Computed tomography (CT) revealed an intraluminal polypoid filling defect arising from the isthmus of the aorta projecting into the proximal descending aorta and findings consistent with infarction of the spleen and right kidney. Infectious, autoimmune, hematologic, and oncologic work-up were all unyielding. The patient was started on heparin and later transitioned to apixaban 5 mg twice a day and 81 mg of aspirin daily. She was also counseled regarding smoking cessation. Two months follow-up CT revealed resolution of the thrombus. Patient had no further thromboembolic complications.
Discussion: We present a unique case of primary aortic thrombus. To our knowledge, this is the first reported case managed successfully with a NOAC. This diagnosis is one of exclusion and through work-up should be completed. Our aim is to raise awareness of this condition and successful management with apixaban in low-risk patients.
Figures



References
-
- Tsilimparis N., Hanack U., Pisimisis G., Yousefi S., Wintzer C., Ruckert R. I. Thrombus in the non-aneurysmal, non-atherosclerotic descending thoracic aorta—an unusual source of arterial embolism. European Journal of Vascular and Endovascular Surgery. 2011;41(4):450–457. doi: 10.1016/j.ejvs.2010.11.004. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
