

Staging System to Predict the Risk of Relapse in Multiple Myeloma Patients Undergoing Autologous Stem Cell Transplantation
- PMID: 31355145
- PMCID: PMC6640159
- DOI: 10.3389/fonc.2019.00633
Staging System to Predict the Risk of Relapse in Multiple Myeloma Patients Undergoing Autologous Stem Cell Transplantation
Abstract
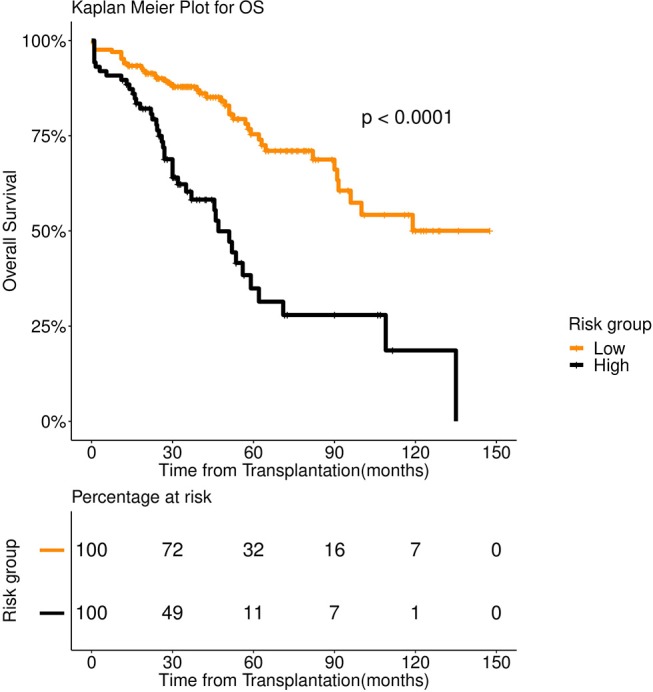
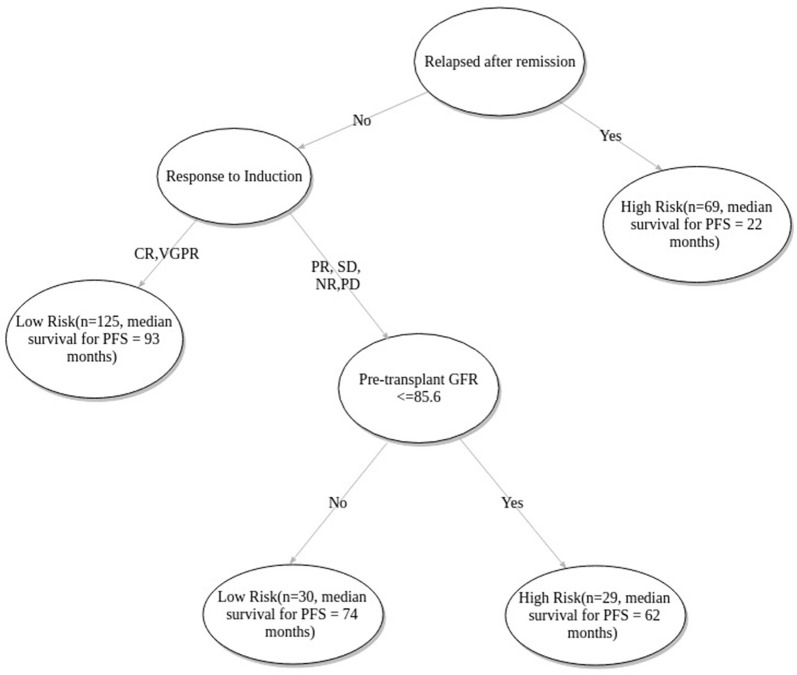
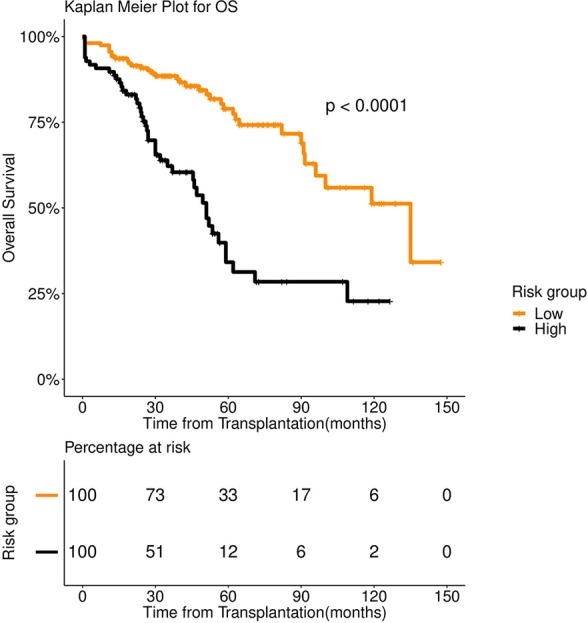
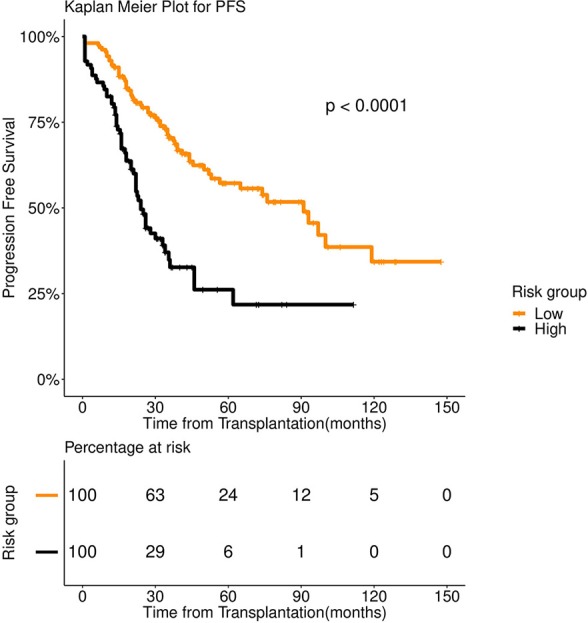
Over the last decade autologous stem cell transplantation (ASCT) has emerged as the standard of care in the management of Multiple Myeloma (MM). However, the cases of early relapse (within 36 months) after the stem cell rescue remains a significant challenge. For a lot of practical purposes, it is crucial to identify whether a patient undergoing ASCT falls into the high-risk group (likely to relapse within 36 months) or a low risk one. Our analysis showed that existing MM staging systems (International Staging System or ISS and Durie Salmon Staging or DSS) are not sufficient to discriminate between the risk groups significantly. To address this, we gathered a total of 39 clinical and laboratory parameters of 347 patients from the Department of Medical Oncology of All India Institute of Medical Sciences (AIIMS). We employed a stacked machine learning model consisting spectral clustering and Fast and Frugal Tree (FFT) technique to come up with a 3-factor multivariate 2-stage staging scheme, which turns out to be extremely decisive about the outcome of the stem cell rescue. Our model comes up with a three-factor (1. if patients has relapsed following remission, 2. response to induction, 3. pre-transplant Glomerular Filtration Rate or GFR) staging scheme. The resulting model stratifies patients into high-risk and low-risk groups with markedly distinct progression-free (median survival-24 months vs. 91 months) and overall survival (median survival-51 months vs. 135 months) patterns.
Keywords: autologous stem cell transplantation; fast and frugal tree; multiple myeloma; multivariate survival analysis; risk of relapse; spectral clustering.
Figures

References
-
- Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. (2017) 3:524–48. 10.1001/jamaoncol.2016.5688 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources