

MR imaging for acute pancreatitis: the current status of clinical applications
- PMID: 31355236
- PMCID: PMC6614331
- DOI: 10.21037/atm.2019.05.37
MR imaging for acute pancreatitis: the current status of clinical applications
Abstract
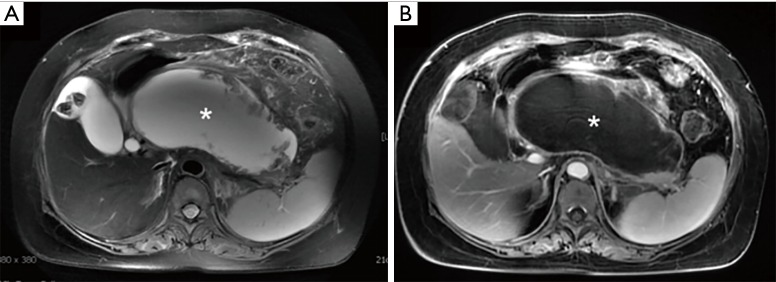
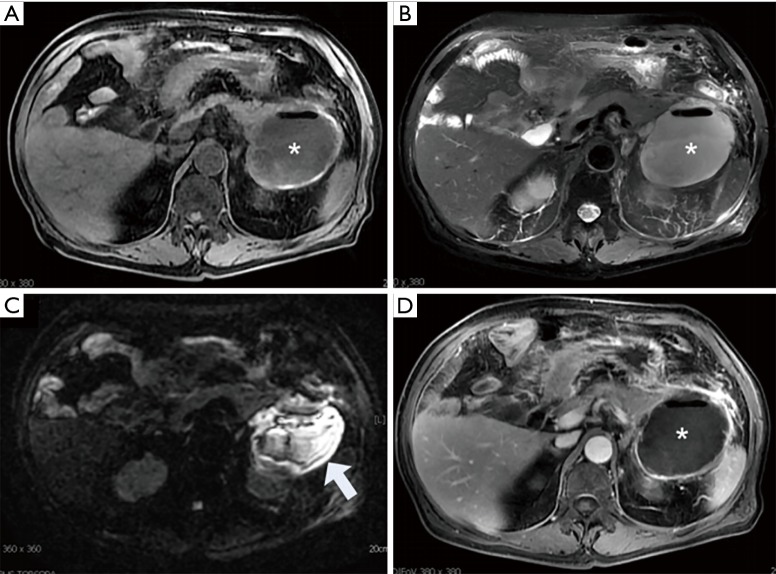
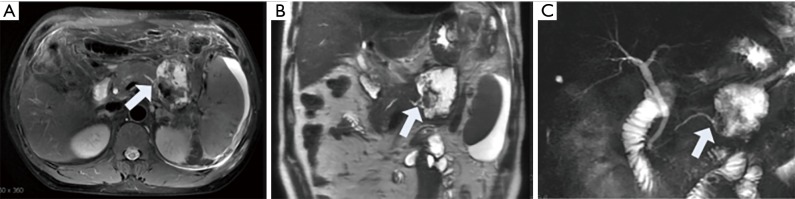
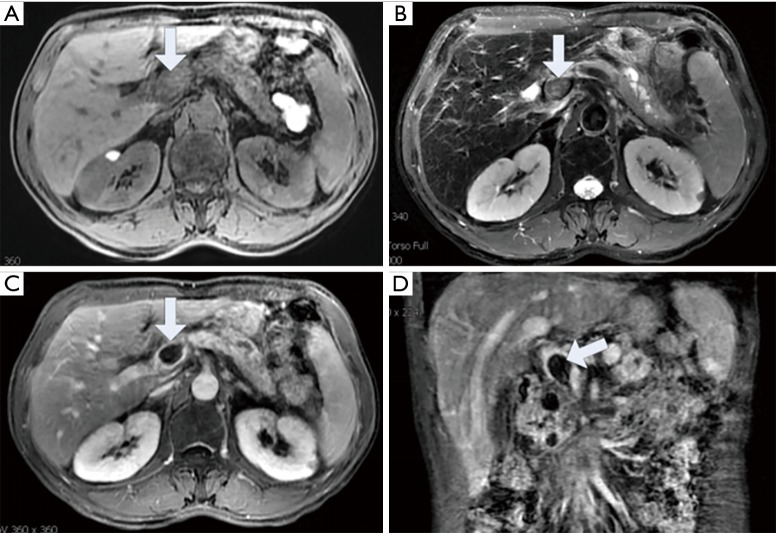
Acute pancreatitis is a common clinical acute abdomen. Imaging examinations play an important role in the management of acute pancreatitis. MR imaging is a noninvasive examination with high tissue contrast and a variety of acquisition sequences that can help determine the diagnosis, complications and severity of acute pancreatitis. The acute pancreatitis classification working group modified the Atlanta classification in 2012 to improve clinical evaluations and standardize the radiologic nomenclature for acute pancreatitis. In particular, the redefinition of necrotizing pancreatitis offers a new understanding of this disease. In clinical practice, there is still a lack of unifying standards between radiologists and physicians, such as for the imaging features of pseudocysts, walled-off necrosis, peripancreatic necrosis and especially for the MR imaging features of acute pancreatitis. In this article, we review the 2012 revised Atlanta classification of acute pancreatitis and recent advances in the clinical applications of MR imaging (MRI) in acute pancreatitis by showing how MRI can provide more optimized information for clinical diagnosis and treatment plan.
Keywords: MR imaging (MRI); acute pancreatitis (AP); local complication.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources