

Association between Blood Potassium Level and Recovery of Postoperative Gastrointestinal Motility during Continuous Renal Replacement Therapy in Patient Undergoing Open Abdominal Surgery
- PMID: 31355273
- PMCID: PMC6634123
- DOI: 10.1155/2019/6392751
Association between Blood Potassium Level and Recovery of Postoperative Gastrointestinal Motility during Continuous Renal Replacement Therapy in Patient Undergoing Open Abdominal Surgery
Abstract
Background: The aim of this study was to identify the blood potassium level beneficial to the postoperative recovery of gastrointestinal motility during continuous renal replacement therapy (CRRT) in patient undergoing open abdominal surgery.
Materials and methods: 538 critically ill patients after open abdominal surgery and receiving CRRT were retrospectively recruited as the study cohort. Demographic and clinical data were recorded along with an evaluation of the postoperative gastrointestinal motility.
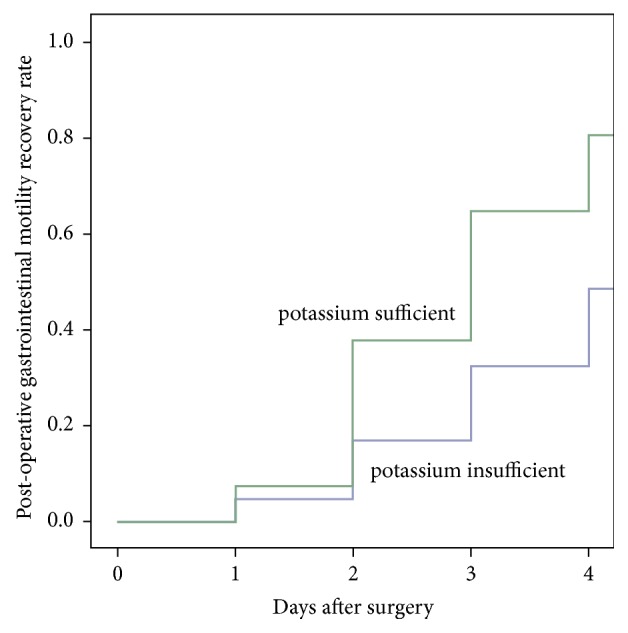
Results: Correlation analysis was used to assess the correlation coefficient, and then the variables with correlation coefficient value less than 0.5 were included in the binary logistic regression model. Binary logistic regression model indicated that the postoperative blood potassium level was independently associated with the recovery of gastrointestinal motility (OR=0.109, 95% CI= 0.063 to 0.190, p<0.001). Based on the normal range of blood potassium level, we selected the cut-off point of blood potassium level via Weight of Evidence analysis, which was 4.00 mmol/L. Compared with the patients with insufficient blood potassium levels (plasma potassium concentration < 4.00 mmol/L), those with sufficient blood potassium levels (plasma potassium concentration≥ 4.00 mmol/L) conferred an increase in the rate of 4-day postoperative recovery of gastrointestinal motility (OR= 4.425, 95% CI = 2.933 to 6.667, p<0.001).
Conclusions: Maintaining the blood potassium concentrations at a relatively high level of the normal blood potassium range during CRRT would be beneficial to postoperative recovery of gastrointestinal motility.
Figures


References
-
- Lobo D. N., Bostock K. A., Neal K. R., Perkins A. C., Rowlands B. J., Allison S. P. Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection: a randomised controlled trial. The Lancet. 2002;359(9320):1812–1818. doi: 10.1016/S0140-6736(02)08711-1. - DOI - PubMed
-
- González-Fajardo J., Mengibar L., Brizuela J., Castrodeza J., Vaquero-Puerta C. Effect of postoperative restrictive fluid therapy in the recovery of patients with abdominal vascular surgery. European Journal of Vascular and Endovascular Surgery. 2009;37(5):538–543. doi: 10.1016/j.ejvs.2009.01.010. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
