

CAR T cells for brain tumors: Lessons learned and road ahead
- PMID: 31355493
- PMCID: PMC6771592
- DOI: 10.1111/imr.12773
CAR T cells for brain tumors: Lessons learned and road ahead
Abstract
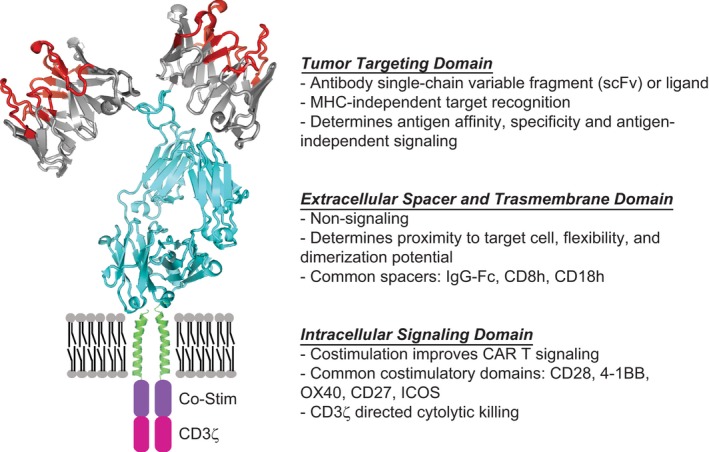
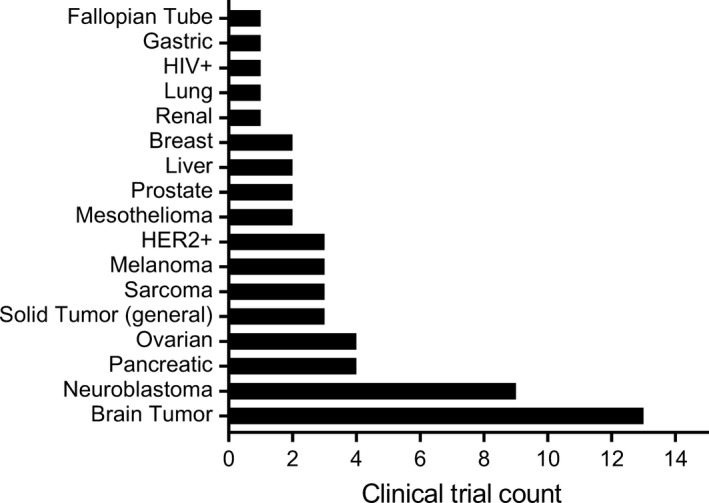
Malignant brain tumors, including glioblastoma, represent some of the most difficult to treat of solid tumors. Nevertheless, recent progress in immunotherapy, across a broad range of tumor types, provides hope that immunological approaches will have the potential to improve outcomes for patients with brain tumors. Chimeric antigen receptors (CAR) T cells, a promising immunotherapeutic modality, utilizes the tumor targeting specificity of any antibody or receptor ligand to redirect the cytolytic potency of T cells. The remarkable clinical response rates of CD19-targeted CAR T cells and early clinical experiences in glioblastoma demonstrating safety and evidence for disease modifying activity support the potential of further advancements ultimately providing clinical benefit for patients. The brain, however, is an immune specialized organ presenting unique and specific challenges to immune-based therapies. Remaining barriers to be overcome for achieving effective CAR T cell therapy in the central nervous system (CNS) include tumor antigenic heterogeneity, an immune-suppressive microenvironment, unique properties of the CNS that limit T cell entry, and risks of immune-based toxicities in this highly sensitive organ. This review will summarize preclinical and clinical data for CAR T cell immunotherapy in glioblastoma and other malignant brain tumors, including present obstacles to advancement.
Keywords: T cells; brain tumors; chimeric antigen receptors; glioblastoma.
© 2019 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Patents associated with CAR design, T cell manufacturing, and delivery have been licensed by Mustang Bio., Inc, for which CEB receives licensing and consulting payments.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
