

Outcomes of Endovascular Thrombectomy vs Medical Management Alone in Patients With Large Ischemic Cores: A Secondary Analysis of the Optimizing Patient's Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) Study
- PMID: 31355873
- PMCID: PMC6664381
- DOI: 10.1001/jamaneurol.2019.2109
Outcomes of Endovascular Thrombectomy vs Medical Management Alone in Patients With Large Ischemic Cores: A Secondary Analysis of the Optimizing Patient's Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) Study
Abstract
Importance: The efficacy and safety of endovascular thrombectomy (EVT) in patients with large ischemic cores remains unknown, to our knowledge.
Objective: To compare outcomes in patients with large ischemic cores treated with EVT and medical management vs medical management alone.
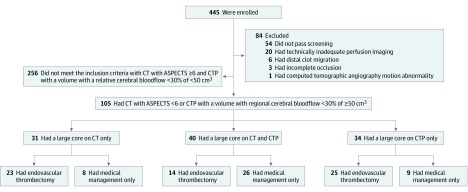
Design, setting, and participants: This prespecified analysis of the Optimizing Patient's Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) trial, a prospective cohort study of imaging selection that was conducted in 9 US comprehensive stroke centers, enrolled patients between January 2016 and February 2018, and followed them up for 90 days. Patients with moderate to severe stroke and anterior circulation large-vessel occlusion presenting up to 24 hours from the time they were last known to be well were eligible for the cohort. Of these, patients with large ischemic cores on computed tomography (CT) (Alberta Stroke Program Early CT Score <6) or CT perfusion scanning (a volume with a relative cerebral blood flow <30% of ≥50 cm3) were included in analyses.
Exposures: Endovascular thrombectomy with medical management (MM) or MM only.
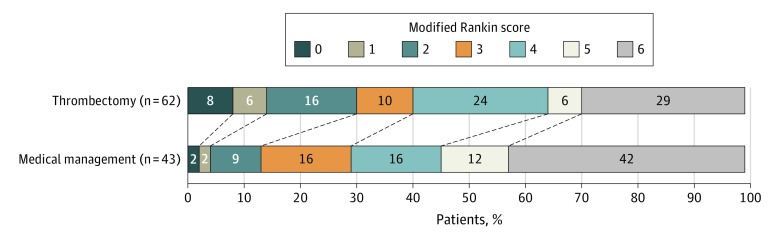
Main outcomes and measures: Functional outcomes at 90 days per modified Rankin scale; safety outcomes (mortality, symptomatic intracerebral hemorrhage, and neurological worsening).
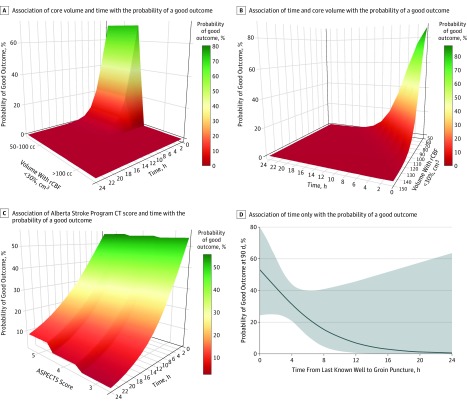
Results: A total of 105 patients with large ischemic cores on either CT or CT perfusion images were included: 71 with Alberta Stroke Program Early CT Scores of 5 or less (EVT, 37; MM, 34), 74 with cores of 50 cm3 or greater on CT perfusion images (EVT, 39; MM, 35), and 40 who had large cores on both CT and CT perfusion images (EVT, 14; MM, 26). The median (interquartile range) age was 66 (60-75) years; 45 patients (43%) were female. Nineteen of 62 patients (31%) who were treated with EVT achieved functional independence (modified Rankin Scale scores, 0-2) vs 6 of 43 patients (14%) treated with MM only (odds ratio [OR], 3.27 [95% CI, 1.11-9.62]; P = .03). Also, EVT was associated with better functional outcomes (common OR, 2.12 [95% CI, 1.05-4.31]; P = .04), less infarct growth (44 vs 98 mL; P = .006), and smaller final infarct volume (97 vs 190 mL; P = .001) than MM. In the odds of functional independence, there was a 42% reduction per 10-cm3 increase in core volume (adjusted OR, 0.58 [95% CI, 0.39-0.87]; P = .007) and a 40% reduction per hour of treatment delay (adjusted OR, 0.60 [95% CI, 0.36-0.99]; P = .045). Of 10 patients who had EVT with core volumes greater than 100 cm3, none had a favorable outcome.
Conclusions and relevance: Although the odds of good outcomes for patients with large cores who receive EVT markedly decline with increasing core size and time to treatment, these data suggest potential benefits. Randomized clinical trials are needed.
Conflict of interest statement
Figures
Comment in
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
