

Current Epidemiology of Surgical Sepsis: Discordance Between Inpatient Mortality and 1-year Outcomes
- PMID: 31356275
- PMCID: PMC6942687
- DOI: 10.1097/SLA.0000000000003458
Current Epidemiology of Surgical Sepsis: Discordance Between Inpatient Mortality and 1-year Outcomes
Abstract
Objective: We sought to compare traditional inpatient outcomes to long-term functional outcomes and mortality of surgical intensive care unit (SICU) patients with sepsis.
Summary of background data: As inpatient sepsis mortality declines, an increasing number of initial sepsis survivors now progress into a state of chronic critical illness (CCI) and their post-discharge outcomes are unclear.
Methods: We performed a prospective, longitudinal cohort study of SICU patients with sepsis.
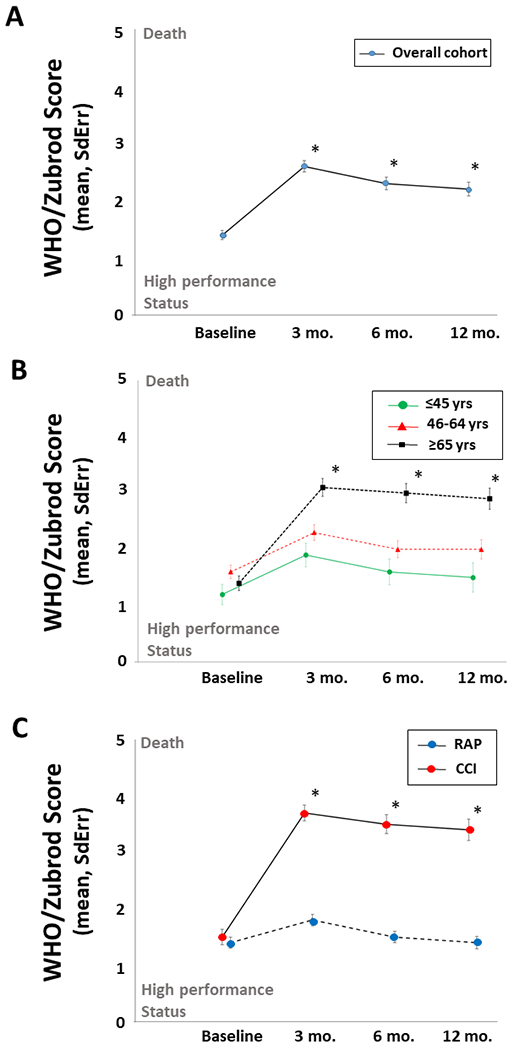
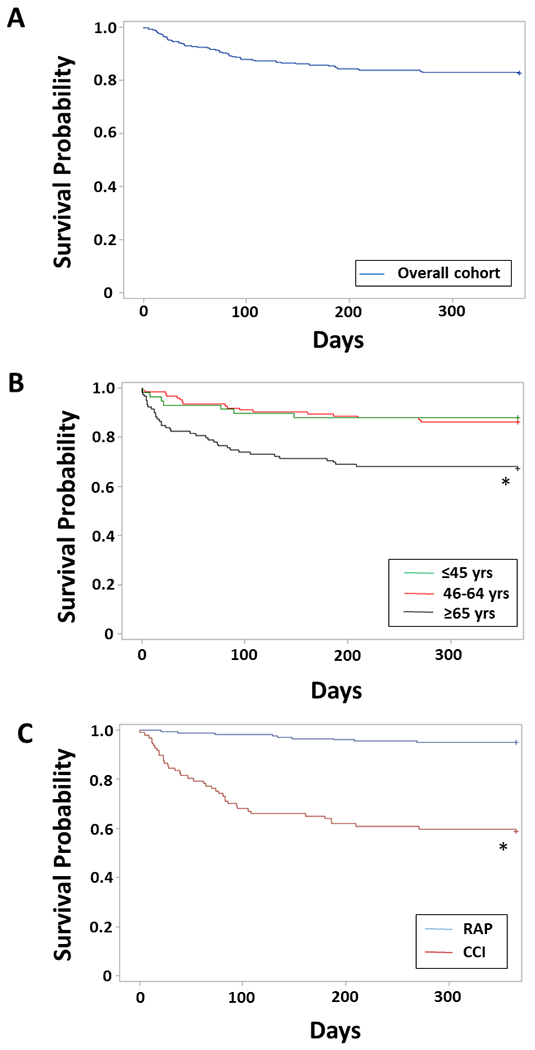
Results: Among this recent cohort of 301 septic SICU patients, 30-day mortality was 9.6%. Only 13 (4%) patients died within 14 days, primarily of refractory multiple organ failure (62%). The majority (n = 189, 63%) exhibited a rapid recovery (RAP), whereas 99 (33%) developed CCI. CCI patients were older, with greater comorbidities, and more severe and persistent organ dysfunction than RAP patients (all P < 0.01). At 12 months, overall cohort performance status was persistently worse than presepsis baseline (WHO/Zubrod score 1.4 ± 0.08 vs 2.2 ± 0.23, P > 0.0001) and mortality was 20.9%. Of note at 12 months, the CCI cohort had persistent severely impaired performance status and a much higher mortality (41.4%) than those with RAP (4.8%) after controlling for age and comorbidity burden (Cox hazard ratio 1.27; 95% confidence interval, 1.14-1.41, P < 0.0001). Among CCI patients, independent risk factors for death by 12 months included severity of comorbidities and persistent organ dysfunction (sequential organ failure assessment ≥6) at day 14 after sepsis onset.
Conclusions: There is discordance between low inpatient mortality and poor long-term outcomes after surgical sepsis, especially among older adults, increasing comorbidity burden and patients that develop CCI. This represents important information when discussing expected outcomes of surgical patients who experience a complicated clinical course owing to sepsis.
Figures
References
-
- Liu V, Escobar GJ, Greene JD, Soule J, Whippy A, Angus DC, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90–2. - PubMed
-
- McKinley BA, Moore LJ, Sucher JF, Todd SR, Turner KL, Valdivia A, et al. Computer protocol facilitates evidence-based care of sepsis in the surgical intensive care unit. J Trauma. 2011;70(5):1153–66; discussion 66–7. - PubMed
-
- Croft CA, Moore FA, Efron PA, Marker PS, Gabrielli A, Westhoff LS, et al. Computer versus paper system for recognition and management of sepsis in surgical intensive care. J Trauma Acute Care Surg. 2014;76(2):311–7; discussion 8–9. - PubMed
-
- Moore LJ, McKinley BA, Turner KL, Todd SR, Sucher JF, Valdivia A, et al. The epidemiology of sepsis in general surgery patients. J Trauma. 2011;70(3):672–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
