

Epidemiology and Outcomes of Cancer-Related Versus Non-Cancer-Related Sepsis Hospitalizations
- PMID: 31356477
- PMCID: PMC6815199
- DOI: 10.1097/CCM.0000000000003896
Epidemiology and Outcomes of Cancer-Related Versus Non-Cancer-Related Sepsis Hospitalizations
Abstract
Objective: Cancer and its treatment are known to be important risk factors for sepsis, contributing to an estimated 12% of U.S. sepsis admissions in the 1990s. However, cancer treatment has evolved markedly over the past 2 decades. We sought to examine how cancer-related sepsis differs from non-cancer-related sepsis.
Design: Observational cohort.
Setting: National Readmissions Database (2013-2014), containing all-payer claims for 49% of U.S.
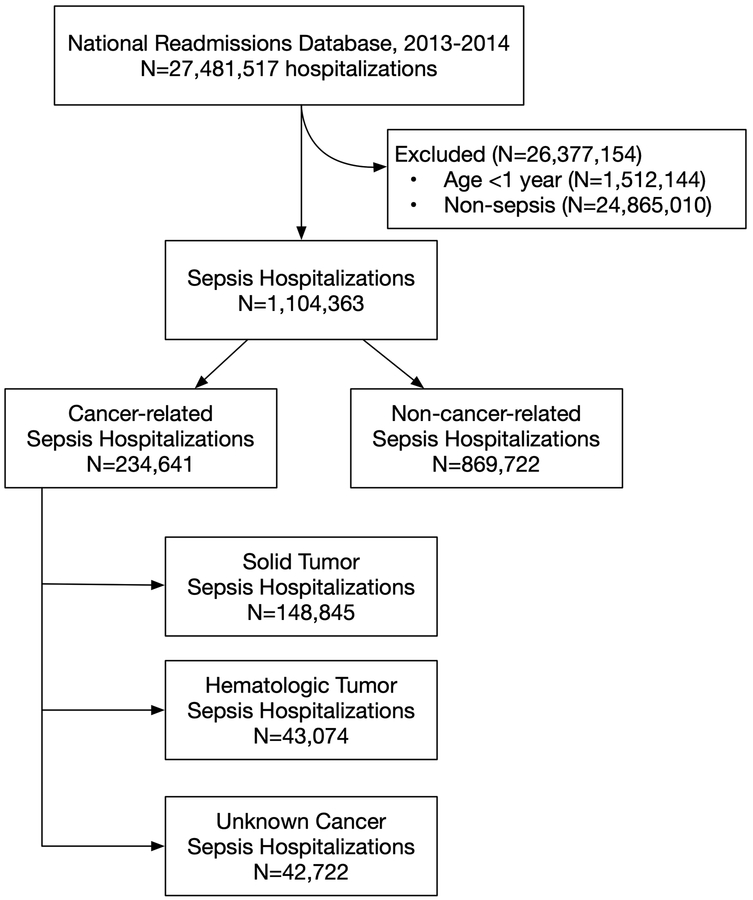
Patients: A total of 1,104,363 sepsis hospitalizations.
Interventions: We identified sepsis hospitalizations in the U.S. National Readmissions Database using explicit codes for severe sepsis, septic shock, or Dombrovskiy criteria (concomitant codes for infection and organ dysfunction). We classified hospitalizations as cancer-related versus non-cancer-related sepsis based on the presence of secondary diagnosis codes for malignancy. We compared characteristics (site of infection and organ dysfunction) and outcomes (in-hospital mortality and 30-d readmissions) of cancer-related versus non-cancer-related sepsis hospitalizations. We also completed subgroup analyses by age, cancer types, and specific cancer diagnoses.
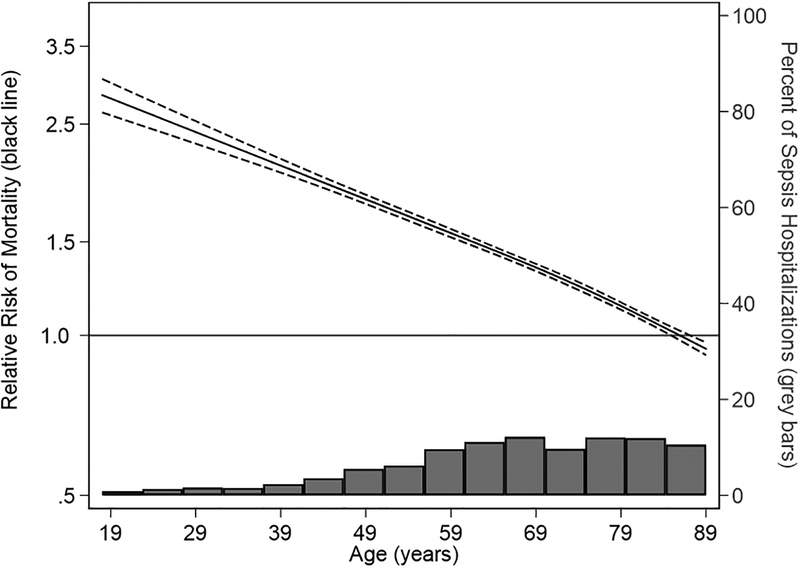
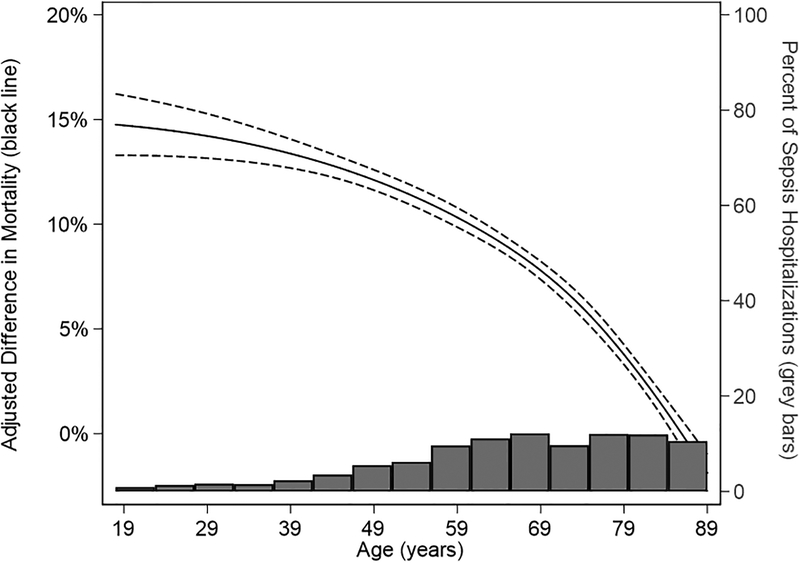
Measurements and main results: There were 27,481,517 hospitalizations in National Readmissions Database 2013-2014, of which 1,104,363 (4.0%) were for sepsis and 4,150,998 (15.1%) were cancer related. In-hospital mortality in cancer-related sepsis was 27.9% versus 19.5% in non-cancer-related sepsis. The median count of organ dysfunctions was indistinguishable, but the rate of specific organ dysfunctions differed by small amounts (e.g., hematologic dysfunction 20.1% in cancer-related sepsis vs 16.6% in non-cancer-related sepsis; p < 0.001). Cancer-related sepsis was associated with an adjusted absolute increase in in-hospital mortality ranging from 2.2% to 15.2% compared with non-cancer-related sepsis. The mortality difference was greatest in younger adults and waned with age. Patients (23.2%) discharged from cancer-related sepsis were rehospitalized within 30 days, compared with 20.1% in non-cancer-related sepsis (p < 0.001).
Conclusions: In this cohort of over 1 million U.S. sepsis hospitalizations, more than one in five were cancer related. The difference in mortality varies substantially across age spectrum and is greatest in younger adults. Readmissions were more common after cancer-related sepsis.
Figures
Comment in
-
Cancer and Sepsis: Adding Insult to Injury-As if Either Alone Were Not Enough?Crit Care Med. 2019 Oct;47(10):1452-1453. doi: 10.1097/CCM.0000000000003950. Crit Care Med. 2019. PMID: 31524693 No abstract available.
References
-
- Fleischmann C, Scherag A, Adhikari NKJ, et al.: Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am J Respir Crit Care Med 2016; 193:259–272 - PubMed
-
- Liu V, Escobar GJ, Greene JD, et al.: Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014; 312:90–92 - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al.: Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001; 29:1303–1310 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
