

Change in left atrial function predicts incident atrial fibrillation: the Multi-Ethnic Study of Atherosclerosis
- PMID: 31356656
- PMCID: PMC6704390
- DOI: 10.1093/ehjci/jez176
Change in left atrial function predicts incident atrial fibrillation: the Multi-Ethnic Study of Atherosclerosis
Abstract
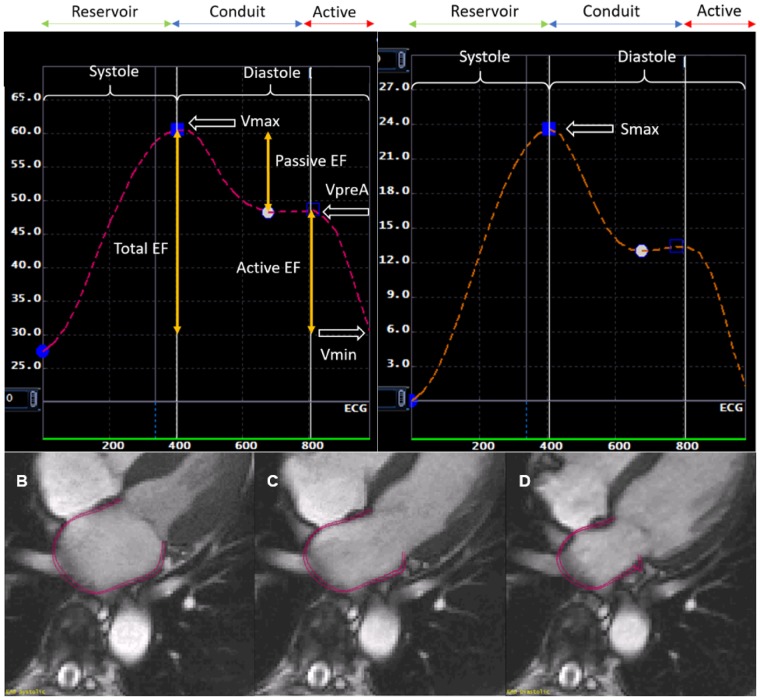
Aims: Longitudinal change in left atrial (LA) structure and function could be helpful in predicting risk for incident atrial fibrillation (AF). We used cardiac magnetic resonance (CMR) imaging to explore the relationship between change in LA structure and function and incident AF in a multi-ethnic population free of clinical cardiovascular disease at baseline.
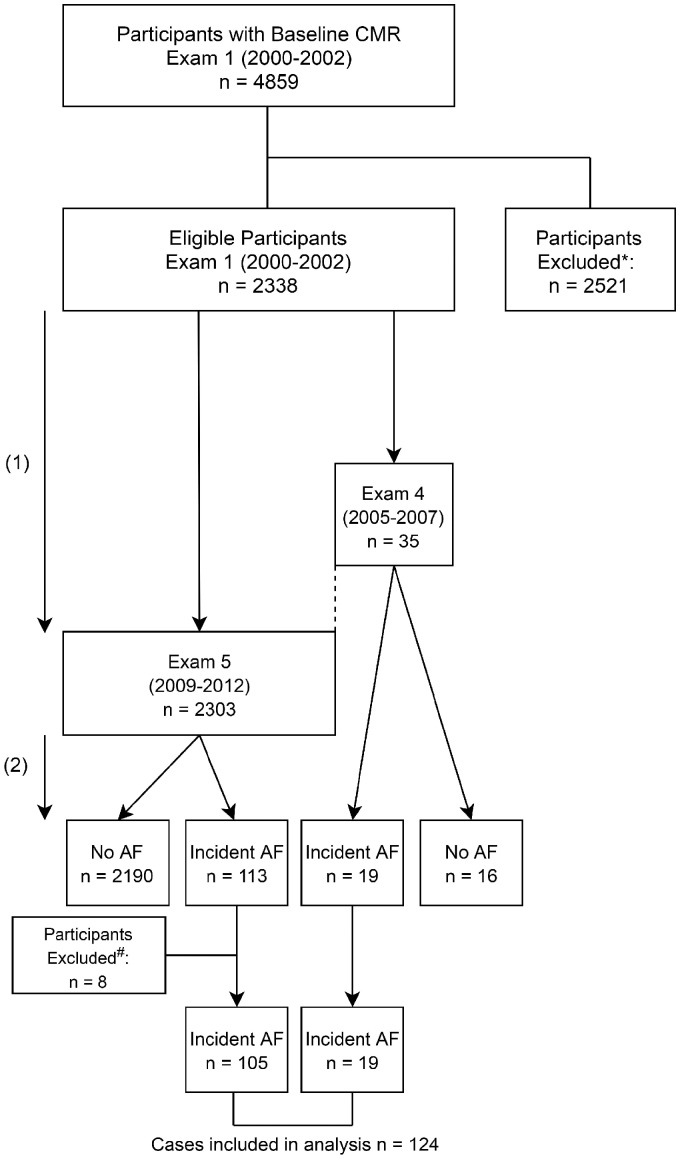
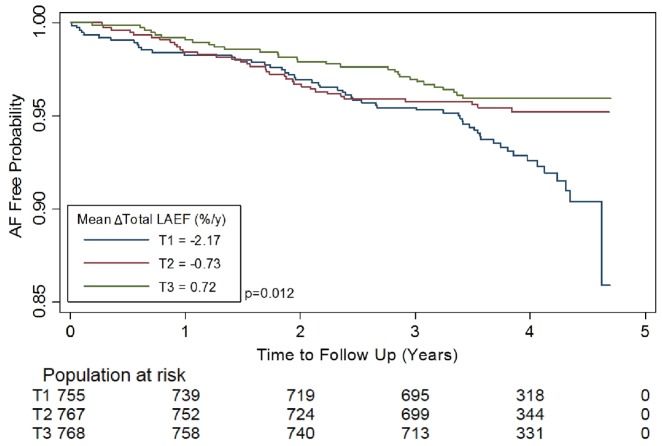
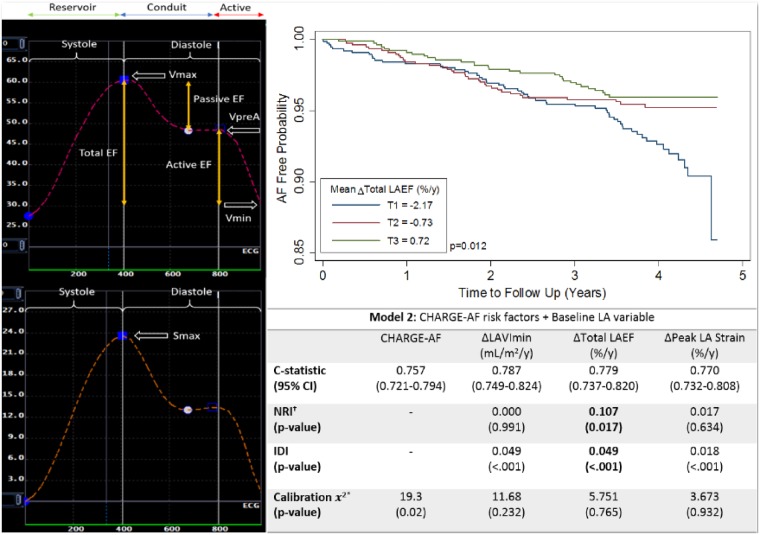
Methods and results: In the Multi-Ethnic Study of Atherosclerosis (MESA), 2338 participants, free at baseline of clinically recognized AF and cardiovascular disease, had LA volume and function assessed with CMR imaging, at baseline (2000-02), and at Exam 4 (2005-07) or 5 (2010-12). Free of AF, 124 participants developed AF over 3.8 ± 0.9 years (2015) following the second imaging. In adjusted Cox regression models, an average annualized change in all LA parameters were significantly associated with an increased risk of AF. An annual decrease of 1-SD unit in total LA emptying fractions (LAEF) was most strongly associated with risk of AF after adjusting for clinical risk factors for AF, baseline LA parameters, and left ventricular mass-to-volume ratio (hazard ratio per SD = 1.91, 95% confidence interval = 1.53-2.38, P < 0.001). The addition of change in total LAEF to an AF risk score improved model discrimination and reclassification (net reclassification improvement = 0.107, P = 0.017; integrative discrimination index = 0.049, P < 0.001).
Conclusion: In this multi-ethnic study population free of clinical cardiovascular disease at baseline, a greater increase in LA volumes and decrease in LA function were associated with incident AF. The addition of change in total LAEF to risk prediction models for AF improved model discrimination and reclassification of AF risk.
Keywords: atrial fibrillation; left atrium.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Clinical factors and imaging leading to risk of incident atrial fibrillation.Eur Heart J Cardiovasc Imaging. 2019 Sep 1;20(9):988-989. doi: 10.1093/ehjci/jez199. Eur Heart J Cardiovasc Imaging. 2019. PMID: 31356655 No abstract available.
Similar articles
-
Change in Left Atrioventricular Coupling Index to Predict Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA).Radiology. 2022 May;303(2):317-326. doi: 10.1148/radiol.210315. Epub 2022 Feb 22. Radiology. 2022. PMID: 35191736 Free PMC article.
-
Cardiac Magnetic Resonance-Measured Left Atrial Volume and Function and Incident Atrial Fibrillation: Results From MESA (Multi-Ethnic Study of Atherosclerosis).Circ Cardiovasc Imaging. 2016 Aug;9(8):10.1161/CIRCIMAGING.115.004299 e004299. doi: 10.1161/CIRCIMAGING.115.004299. Circ Cardiovasc Imaging. 2016. PMID: 27511974 Free PMC article.
-
Left Atrial Mechanical Function and Incident Ischemic Cerebrovascular Events Independent of AF: Insights From the MESA Study.JACC Cardiovasc Imaging. 2019 Dec;12(12):2417-2427. doi: 10.1016/j.jcmg.2019.02.021. Epub 2019 Apr 17. JACC Cardiovasc Imaging. 2019. PMID: 31005519 Free PMC article.
-
Association of right atrial structure with incident atrial fibrillation: a longitudinal cohort cardiovascular magnetic resonance study from the Multi-Ethnic Study of Atherosclerosis (MESA).J Cardiovasc Magn Reson. 2020 May 21;22(1):36. doi: 10.1186/s12968-020-00631-1. J Cardiovasc Magn Reson. 2020. PMID: 32434529 Free PMC article.
-
Change in left atrial function and volume predicts incident heart failure with preserved and reduced ejection fraction: Multi-Ethnic Study of Atherosclerosis.Eur Heart J Cardiovasc Imaging. 2024 Oct 30;25(11):1577-1587. doi: 10.1093/ehjci/jeae138. Eur Heart J Cardiovasc Imaging. 2024. PMID: 38885142 Free PMC article.
Cited by
-
Change in Left Atrioventricular Coupling Index to Predict Incident Atrial Fibrillation: The Multi-Ethnic Study of Atherosclerosis (MESA).Radiology. 2022 May;303(2):317-326. doi: 10.1148/radiol.210315. Epub 2022 Feb 22. Radiology. 2022. PMID: 35191736 Free PMC article.
-
The Palma Echo Platform: Rationale and Design of an Echocardiography Core Lab.Front Cardiovasc Med. 2022 Jun 21;9:909347. doi: 10.3389/fcvm.2022.909347. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35800168 Free PMC article.
-
Atrial cardiomyopathy revisited-evolution of a concept: a clinical consensus statement of the European Heart Rhythm Association (EHRA) of the ESC, the Heart Rhythm Society (HRS), the Asian Pacific Heart Rhythm Society (APHRS), and the Latin American Heart Rhythm Society (LAHRS).Europace. 2024 Aug 30;26(9):euae204. doi: 10.1093/europace/euae204. Europace. 2024. PMID: 39077825 Free PMC article.
-
Evaluating Incident Atrial Fibrillation and Incident Heart Failure as Time-varying Covariates for Time-to-Event Analysis Among Adults 55 Years and Older in the Multi-Ethnic Study of Atherosclerosis (MESA).J Card Fail. 2025 Feb 3:S1071-9164(25)00045-4. doi: 10.1016/j.cardfail.2025.01.012. Online ahead of print. J Card Fail. 2025. PMID: 39909110 Free PMC article.
-
Left Atrioventricular Coupling Index to Predict Incident Heart Failure: The Multi-Ethnic Study of Atherosclerosis.Front Cardiovasc Med. 2021 Sep 1;8:704611. doi: 10.3389/fcvm.2021.704611. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34540915 Free PMC article.
References
-
- Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS.. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation 2004;110:1042–6. - PubMed
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV. et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370. 5. - PubMed
-
- Brambatti M, Connolly SJ, Gold MR, Morillo CA, Capucci A, Muto C. et al. Temporal relationship between subclinical atrial fibrillation and embolic events. Circulation 2014;129:2094–9. - PubMed
-
- Anter E, Jessup M, Callans DJ.. Atrial fibrillation and heart failure: treatment considerations for a dual epidemic. Circulation 2009;119:2516–25. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- R01 HL127659/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- P30 AG049638/AG/NIA NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
