

High FREM2 Gene and Protein Expression Are Associated with Favorable Prognosis of IDH-WT Glioblastomas
- PMID: 31357584
- PMCID: PMC6721429
- DOI: 10.3390/cancers11081060
High FREM2 Gene and Protein Expression Are Associated with Favorable Prognosis of IDH-WT Glioblastomas
Abstract
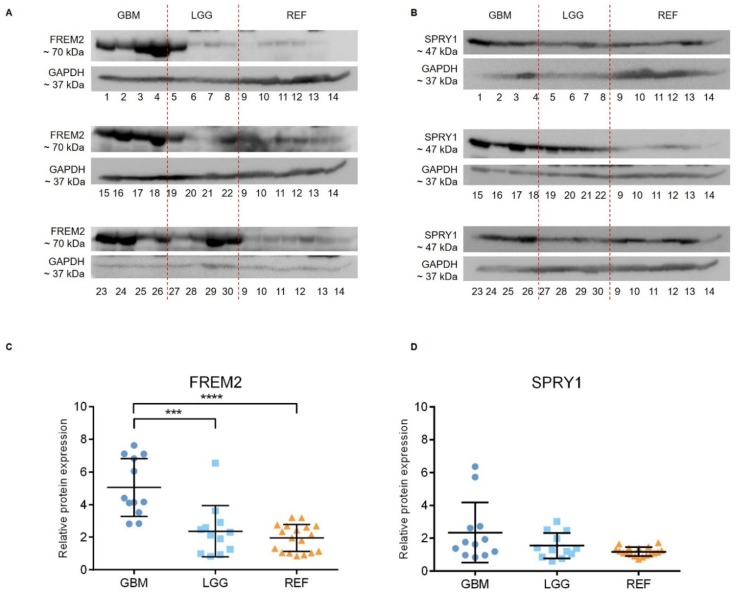
World Health Organization grade IV diffuse gliomas, known as glioblastomas, are the most common malignant brain tumors, and they show poor prognosis. Multimodal treatment of surgery followed by radiation and chemotherapy is not sufficient to increase patient survival, which is 12 to 18 months after diagnosis. Despite extensive research, patient life expectancy has not significantly improved over the last decade. Previously, we identified FREM2 and SPRY1 as genes with differential expression in glioblastoma cell lines compared to nonmalignant astrocytes. In addition, the FREM2 and SPRY1 proteins show specific localization on the surface of glioblastoma cells. In this study, we explored the roles of the FREM2 and SPRY1 genes and their proteins in glioblastoma pathology using human tissue samples. We used proteomic, transcriptomic, and bioinformatics approaches to detect changes at different molecular levels. We demonstrate increased FREM2 protein expression levels in glioblastomas compared to reference samples. At the transcriptomic level, both FREM2 and SPRY1 show increased expression in tissue samples of different glioma grades compared to nonmalignant brain tissue. To broaden our experimental findings, we analyzed The Cancer Genome Atlas glioblastoma patient datasets. We discovered higher FREM2 and SPRY1 gene expression levels in glioblastomas compared to lower grade gliomas and reference samples. In addition, we observed that low FREM2 expression was associated with progression of IDH-mutant low-grade glioma patients. Multivariate analysis showed positive association between FREM2 and favorable prognosis of IDH-wild type glioblastoma. We conclude that FREM2 has an important role in malignant progression of glioblastoma, and we suggest deeper analysis to determine its involvement in glioblastoma pathology.
Keywords: FREM2; SPRY1; TCGA; glioblastoma; malignancy.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures






Similar articles
-
Algorithmically Deduced FREM2 Molecular Pathway Is a Potent Grade and Survival Biomarker of Human Gliomas.Cancers (Basel). 2021 Aug 16;13(16):4117. doi: 10.3390/cancers13164117. Cancers (Basel). 2021. PMID: 34439271 Free PMC article.
-
Meta-Analysis and Experimental Validation Identified FREM2 and SPRY1 as New Glioblastoma Marker Candidates.Int J Mol Sci. 2018 May 4;19(5):1369. doi: 10.3390/ijms19051369. Int J Mol Sci. 2018. PMID: 29734672 Free PMC article.
-
Reclassification of TCGA Diffuse Glioma Profiles Linked to Transcriptomic, Epigenetic, Genomic and Clinical Data, According to the 2021 WHO CNS Tumor Classification.Int J Mol Sci. 2022 Dec 21;24(1):157. doi: 10.3390/ijms24010157. Int J Mol Sci. 2022. PMID: 36613601 Free PMC article.
-
Advanced Magnetic Resonance Imaging in Pediatric Glioblastomas.Front Neurol. 2021 Nov 10;12:733323. doi: 10.3389/fneur.2021.733323. eCollection 2021. Front Neurol. 2021. PMID: 34858308 Free PMC article. Review.
-
Overcoming the blood-brain tumor barrier for effective glioblastoma treatment.Drug Resist Updat. 2015 Mar;19:1-12. doi: 10.1016/j.drup.2015.02.002. Epub 2015 Mar 6. Drug Resist Updat. 2015. PMID: 25791797 Review.
Cited by
-
Case of multifocal glioblastoma with four fusion transcripts of ALK, FGFR2, NTRK2, and NTRK3 genes stresses the need for tumor tissue multisampling for transcriptomic analysis.Cold Spring Harb Mol Case Stud. 2021 Aug 2;7(4):a006100. doi: 10.1101/mcs.a006100. Print 2021 Aug. Cold Spring Harb Mol Case Stud. 2021. PMID: 34341009 Free PMC article.
-
Identification of Tumor Microenvironment-Related Prognostic Biomarkers for Ovarian Serous Cancer 3-Year Mortality Using Targeted Maximum Likelihood Estimation: A TCGA Data Mining Study.Front Genet. 2021 Jun 3;12:625145. doi: 10.3389/fgene.2021.625145. eCollection 2021. Front Genet. 2021. PMID: 34149794 Free PMC article.
-
Metabolic-related gene pairs signature analysis identifies ABCA1 expression levels on tumor-associated macrophages as a prognostic biomarker in primary IDHWT glioblastoma.Front Immunol. 2022 Sep 30;13:869061. doi: 10.3389/fimmu.2022.869061. eCollection 2022. Front Immunol. 2022. PMID: 36248907 Free PMC article.
-
Association of a Novel DOCK2 Mutation-Related Gene Signature With Immune in Hepatocellular Carcinoma.Front Genet. 2022 May 10;13:872224. doi: 10.3389/fgene.2022.872224. eCollection 2022. Front Genet. 2022. PMID: 35620462 Free PMC article.
-
Algorithmically Deduced FREM2 Molecular Pathway Is a Potent Grade and Survival Biomarker of Human Gliomas.Cancers (Basel). 2021 Aug 16;13(16):4117. doi: 10.3390/cancers13164117. Cancers (Basel). 2021. PMID: 34439271 Free PMC article.
References
-
- Louis D.N., Perry A., Reifenberger G., von Deimling A., Figarella-Branger D., Cavenee W.K., Ohgaki H., Wiestler O.D., Kleihues P., Ellison D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
