

Robot-assisted gait training for balance and lower extremity function in patients with infratentorial stroke: a single-blinded randomized controlled trial
- PMID: 31358017
- PMCID: PMC6664752
- DOI: 10.1186/s12984-019-0553-5
Robot-assisted gait training for balance and lower extremity function in patients with infratentorial stroke: a single-blinded randomized controlled trial
Abstract
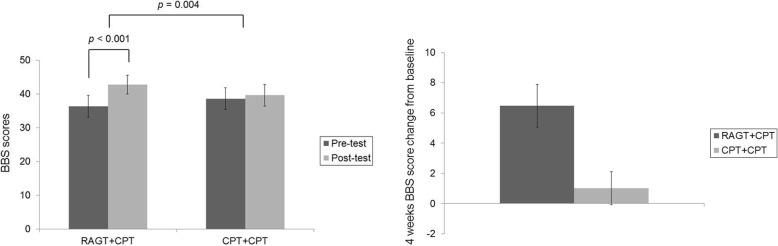
Background: Balance impairments are common in patients with infratentorial stroke. Although robot-assisted gait training (RAGT) exerts positive effects on balance among patients with stroke, it remains unclear whether such training is superior to conventional physical therapy (CPT). Therefore, we aimed to investigate the effects of RAGT combined with CPT and compared them with the effects of CPT only on balance and lower extremity function among survivors of infratentorial stroke.
Methods: This study was a single-blinded, randomized controlled trial with a crossover design conducted at a single rehabilitation hospital. Patients (n = 19; 16 men, three women; mean age: 47.4 ± 11.6 years) with infratentorial stroke were randomly allocated to either group A (4 weeks of RAGT+CPT, followed by 4 weeks of CPT+CPT) or group B (4 weeks of CPT+CPT followed by 4 weeks of RAGT+CPT). Changes in dynamic and static balance as indicated by Berg Balance Scale scores were regarded as the primary outcome measure. Outcome measures were evaluated for each participant at baseline and after each 4-week intervention period.
Results: No significant differences in outcome-related variables were observed between group A and B at baseline. In addition, no significant time-by-group interactions were observed for any variables, indicating that intervention order had no effect on lower extremity function or balance. Significantly greater improvements in secondary functional outcomes such as lower extremity Fugl-Meyer assessment (FMA-LE) and scale for the assessment and rating of ataxia (SARA) were observed following the RAGT+CPT intervention than following the CPT+CPT intervention.
Conclusion: RAGT produces clinically significant improvements in balance and lower extremity function in individuals with infratentorial stroke. Thus, RAGT may be useful for patients with balance impairments secondary to other pathologies.
Trial registration: ClinicalTrials.gov Identifier NCT02680691. Registered 09 February 2016; retrospectively registered.
Keywords: Balance; Gait impairment; Robot-assisted gait training; Stroke.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Harris JE, Eng JJ, Marigold DS, Tokuno CD, Louis CS. Relationship of balance and mobility to fall incidence in people with chronic stroke. Phys Ther. 2005;85:150–158. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
