

Effects of testosterone supplementation on body composition and lower-body muscle function during severe exercise- and diet-induced energy deficit: A proof-of-concept, single centre, randomised, double-blind, controlled trial
- PMID: 31358477
- PMCID: PMC6711889
- DOI: 10.1016/j.ebiom.2019.07.059
Effects of testosterone supplementation on body composition and lower-body muscle function during severe exercise- and diet-induced energy deficit: A proof-of-concept, single centre, randomised, double-blind, controlled trial
Abstract
Background: Severe energy deficits during military operations, produced by significant increases in exercise and limited dietary intake, result in conditions that degrade lean body mass and lower-body muscle function, which may be mediated by concomitant reductions in circulating testosterone.
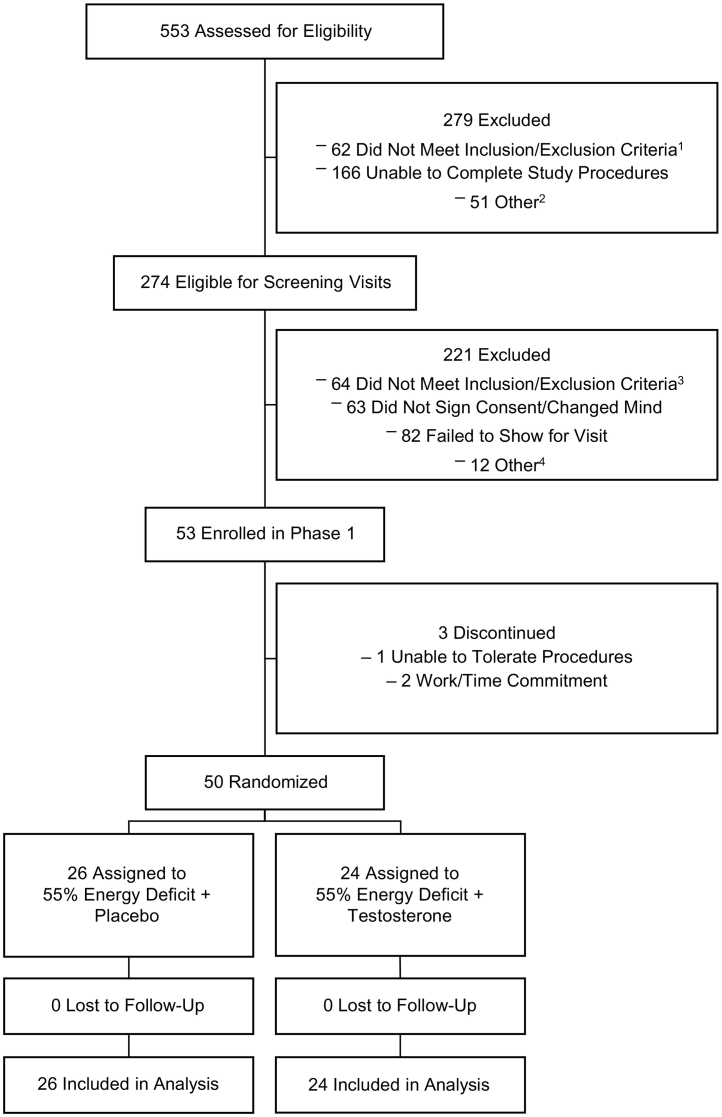
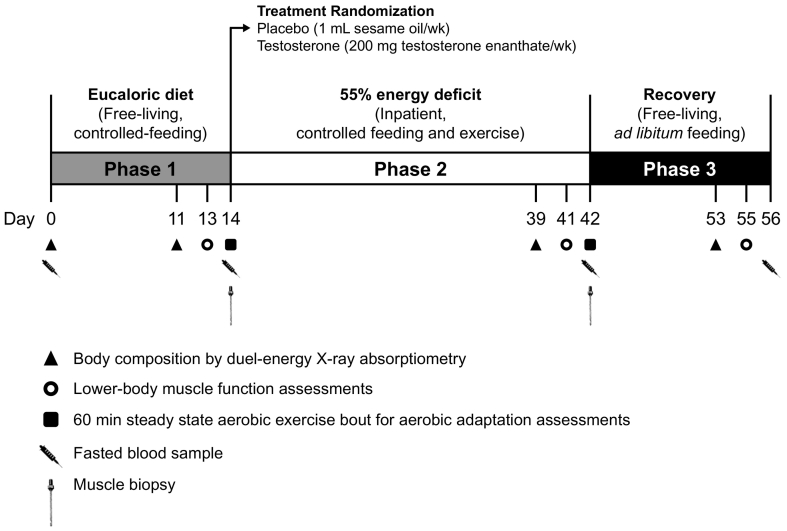
Methods: We conducted a three-phase, proof-of-concept, single centre, randomised, double-blind, placebo-controlled trial (CinicalTrials.gov, NCT02734238) of non-obese men: 14-d run-in, free-living, eucaloric diet phase; 28-d live-in, 55% exercise- and diet-induced energy deficit phase with (200 mg testosterone enanthate per week, Testosterone, n = 24) or without (Placebo, n = 26) exogenous testosterone; and 14-d recovery, free-living, ad libitum diet phase. Body composition was the primary end point; secondary endpoints included lower-body muscle function and health-related biomarkers.
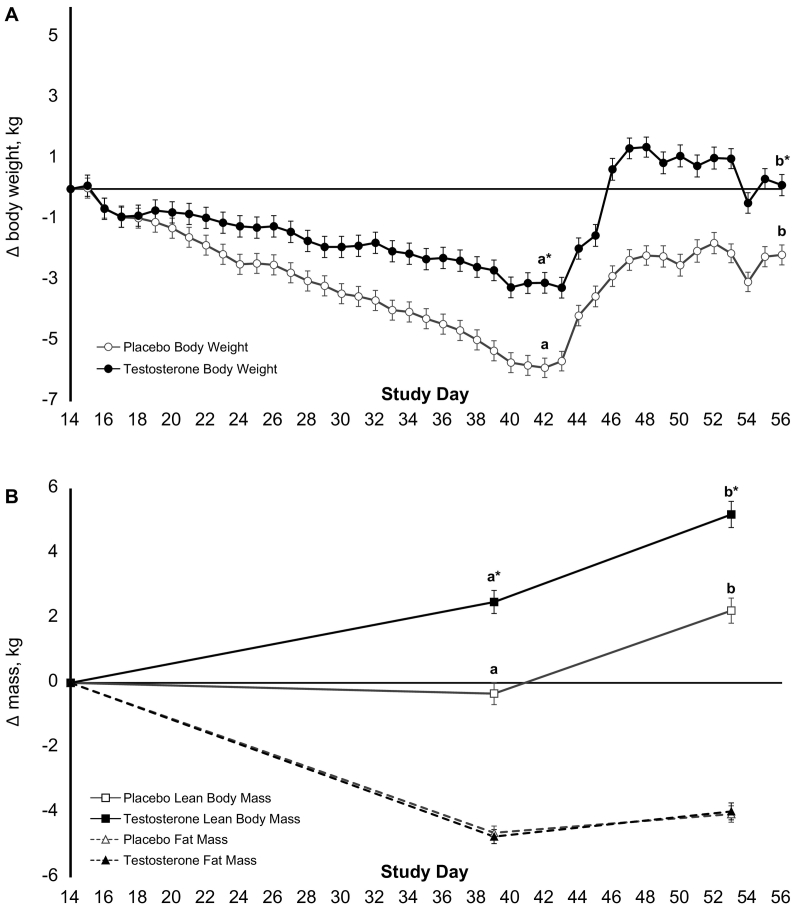
Findings: Following energy deficit, lean body mass increased in Testosterone and remained stable in Placebo, such that lean body mass significantly differed between groups [mean difference between groups (95% CI), 2.5 kg (3.3, 1.6); P < .0001]. Fat mass decreased similarly in both treatment groups [0.2 (-0.4, 0.7), P = 1]. Change in lean body mass was associated with change in total testosterone (r = 0.71, P < .0001). Supplemental testosterone had no effect on lower-body muscle function or health-related biomarkers.
Interpretation: Findings suggest that supplemental testosterone may increase lean body mass during short-term severe energy deficit in non-obese, young men, but it does not appear to attenuate lower-body functional decline.
Funding: Collaborative Research to Optimize Warfighter Nutrition projects I and II, Joint Program Committee-5, funded by the US Department of Defence.
Keywords: Anabolism; Hypogonadism; Hypothalamic-pituitary-gonadal axis; Lower-body muscle function; Military operational stress; Muscle mass; Semi-starvation.
Copyright © 2019. Published by Elsevier B.V.
Conflict of interest statement
J.C.W., O.T.C., and K.M.G. reported that their institution received funding from the US Department of Defence for work associated with this publication. H.R.L. reported receiving personal fees from Pfizer, Inc., for work outside this publication. All remaining authors declare no competing interests. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Army or the Department of Defence. Any citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement of approval of the products or services of these organizations.
Figures
Comment in
-
Testosterone replacement for male military personnel - A potential countermeasure to reduce injury and improve performance under extreme conditions.EBioMedicine. 2019 Sep;47:16-17. doi: 10.1016/j.ebiom.2019.08.015. Epub 2019 Aug 10. EBioMedicine. 2019. PMID: 31405757 Free PMC article. No abstract available.
References
-
- Friedl K.E., Moore R.J., Hoyt R.W., Marchitelli L.J., Martinez-Lopez L.E., Askew E.W. Endocrine markers of semistarvation in healthy lean men in a multistressor environment. J Appl Physiol (1985) 2000;88(5):1820–1830. - PubMed
-
- Nindl B.C., Friedl K.E., Frykman P.N., Marchitelli L.J., Shippee R.L., Patton J.F. Physical performance and metabolic recovery among lean, healthy men following a prolonged energy deficit. Int J Sports Med. 1997;18(5):317–324. - PubMed
-
- Murphy N.E., Carrigan C.T., Karl J.P., Pasiakos S.M., Margolis L.M. Threshold of energy deficit and lower-body performance declines in military personnel: a meta-regression. Sports Med. Sep 2018;48(9):2169–2178. (Review) - PubMed
-
- Henning P.C., Park B.S., Kim J.S. Physiological decrements during sustained military operational stress. Mil Med. 2011;176(9):991–997. - PubMed
-
- Berryman C.E., Young A.J., Karl J.P., Kenefick R.W., Margolis L.M., Cole R.E. Severe negative energy balance during 21 d at high altitude decreases fat-free mass regardless of dietary protein intake: a randomized controlled trial. FASEB J. 2018;32(2):894–905. - PubMed
