

Treatment with Next-Generation ALK Inhibitors Fuels Plasma ALK Mutation Diversity
- PMID: 31358542
- PMCID: PMC6858956
- DOI: 10.1158/1078-0432.CCR-19-1436
Treatment with Next-Generation ALK Inhibitors Fuels Plasma ALK Mutation Diversity
Abstract
Purpose: Acquired resistance to next-generation ALK tyrosine kinase inhibitors (TKIs) is often driven by secondary ALK mutations. Here, we investigated utility of plasma genotyping for identifying ALK resistance mutations at relapse on next-generation ALK TKIs.
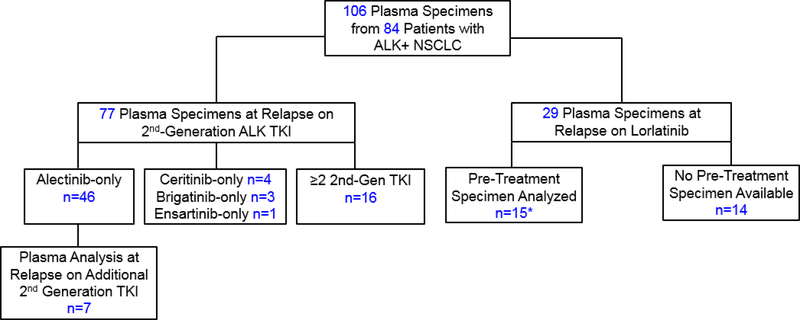
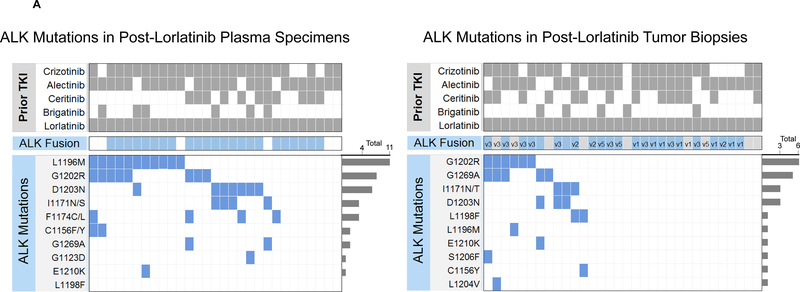
Experimental design: We analyzed 106 plasma specimens from 84 patients with advanced ALK-positive lung cancer treated with second- and third-generation ALK TKIs using a commercially available next-generation sequencing (NGS) platform (Guardant360). Tumor biopsies from TKI-resistant lesions underwent targeted NGS to identify ALK mutations.
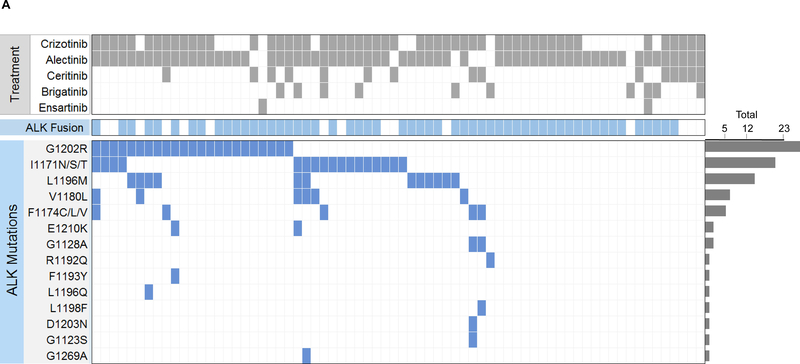
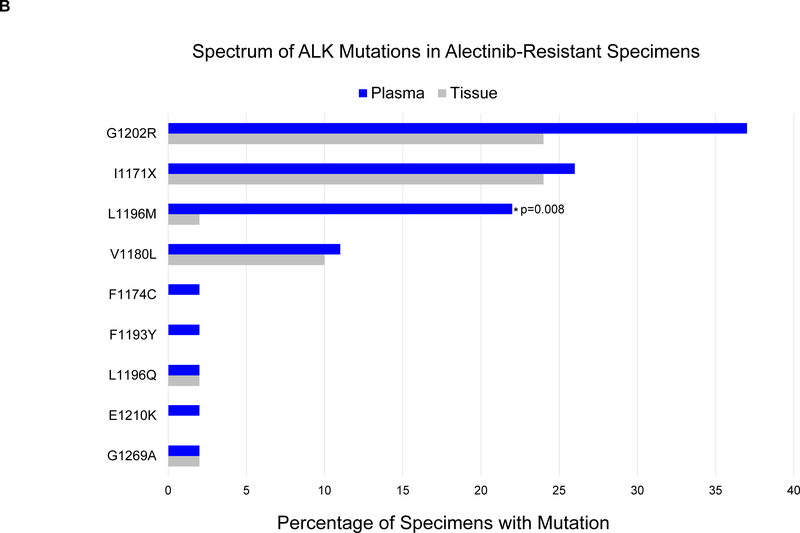
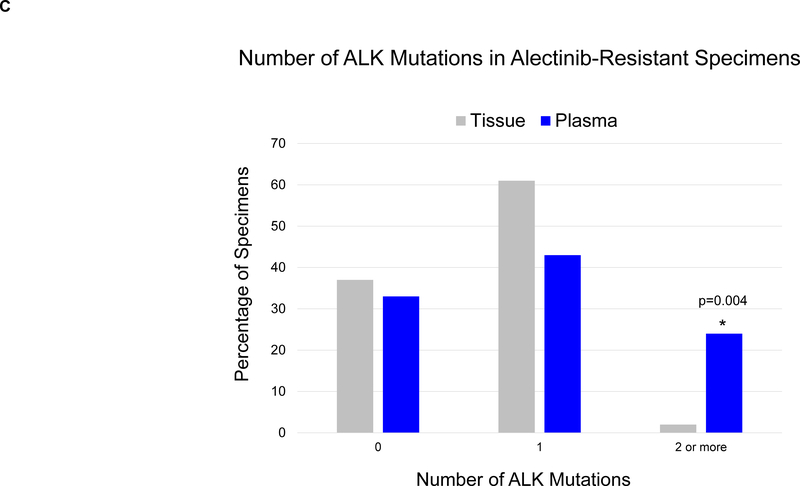
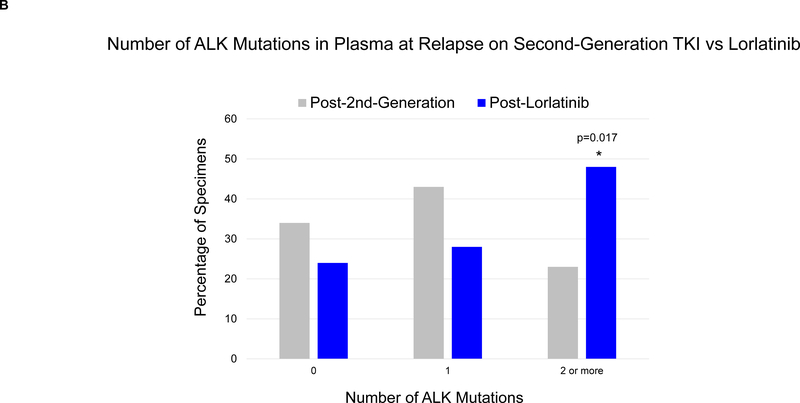
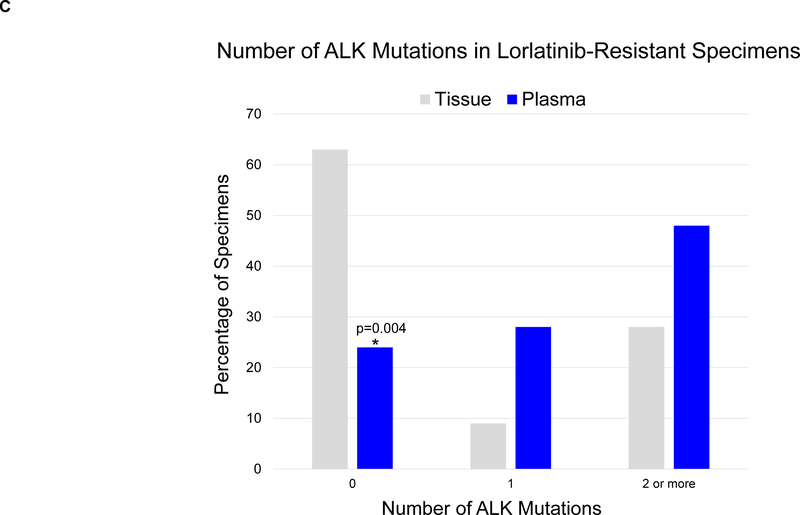
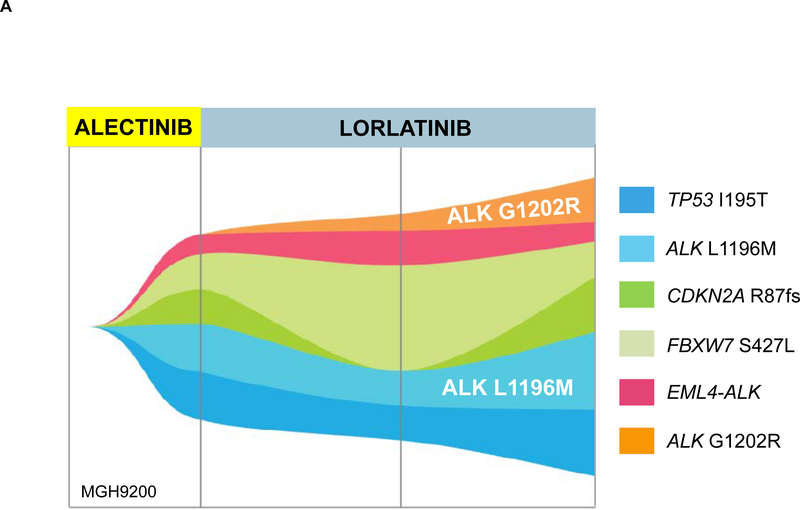
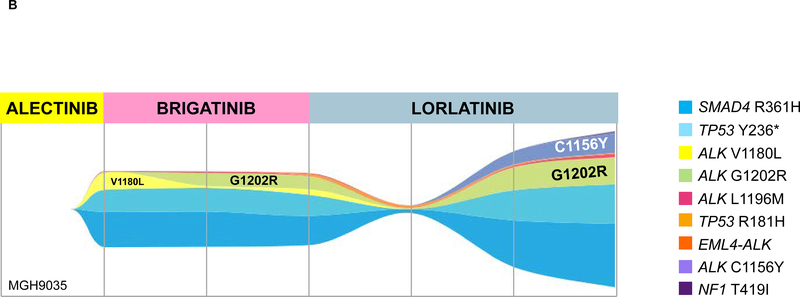
Results: By genotyping plasma, we detected an ALK mutation in 46 (66%) of 70 patients relapsing on a second-generation ALK TKI. When post-alectinib plasma and tumor specimens were compared, there was no difference in frequency of ALK mutations (67% vs. 63%), but plasma specimens were more likely to harbor ≥2 ALK mutations (24% vs. 2%, P = 0.004). Among 29 patients relapsing on lorlatinib, plasma genotyping detected an ALK mutation in 22 (76%), including 14 (48%) with ≥2 ALK mutations. The most frequent combinations of ALK mutations were G1202R/L1196M and D1203N/1171N. Detection of ≥2 ALK mutations was significantly more common in patients relapsing on lorlatinib compared with second-generation ALK TKIs (48% vs. 23%, P = 0.017). Among 15 patients who received lorlatinib after a second-generation TKI, serial plasma analysis demonstrated that eight (53%) acquired ≥1 new ALK mutations on lorlatinib.
Conclusions: ALK resistance mutations increase with each successive generation of ALK TKI and may be underestimated by tumor genotyping. Sequential treatment with increasingly potent ALK TKIs may promote acquisition of ALK resistance mutations leading to treatment-refractory compound ALK mutations.
©2019 American Association for Cancer Research.
Figures
References
-
- Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448(7153):561–566. - PubMed
-
- Soria JC, Tan DS, Chiari R, et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): a randomised, open-label, phase 3 study. Lancet. 2017;389(10072):917–929. - PubMed
-
- Peters S, Camidge DR, Shaw AT, et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2017. - PubMed
-
- Camidge DR, Kim HR, Ahn MJ, et al. Brigatinib versus Crizotinib in ALK-Positive Non-Small-Cell Lung Cancer. N Engl J Med. 2018;379(21):2027–2039. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
