

Association between complications and death within 30 days after noncardiac surgery
- PMID: 31358597
- PMCID: PMC6663503
- DOI: 10.1503/cmaj.190221
Association between complications and death within 30 days after noncardiac surgery
Abstract
Background: Among adults undergoing contemporary noncardiac surgery, little is known about the frequency and timing of death and the associations between perioperative complications and mortality. We aimed to establish the frequency and timing of death and its association with perioperative complications.
Methods: We conducted a prospective cohort study of patients aged 45 years and older who underwent inpatient noncardiac surgery at 28 centres in 14 countries. We monitored patients for complications until 30 days after surgery and determined the relation between these complications and 30-day mortality using a Cox proportional hazards model.
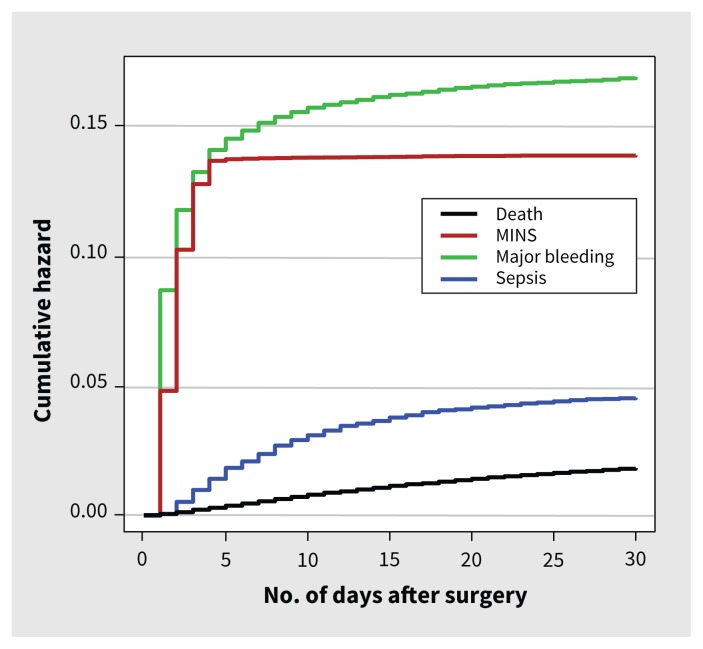
Results: We included 40 004 patients. Of those, 715 patients (1.8%) died within 30 days of surgery. Five deaths (0.7%) occurred in the operating room, 500 deaths (69.9%) occurred after surgery during the index admission to hospital and 210 deaths (29.4%) occurred after discharge from the hospital. Eight complications were independently associated with 30-day mortality. The 3 complications with the largest attributable fractions (AF; i.e., potential proportion of deaths attributable to these complications) were major bleeding (6238 patients, 15.6%; adjusted hazard ratio [HR] 2.6, 95% confidence interval [CI] 2.2-3.1; AF 17.0%); myocardial injury after noncardiac surgery [MINS] (5191 patients, 13.0%; adjusted HR 2.2, 95% CI 1.9-2.6; AF 15.9%); and sepsis (1783 patients, 4.5%; adjusted HR 5.6, 95% CI 4.6-6.8; AF 12.0%).
Interpretation: Among adults undergoing noncardiac surgery, 99.3% of deaths occurred after the procedure and 44.9% of deaths were associated with 3 complications: major bleeding, MINS and sepsis. Given these findings, focusing on the prevention, early identification and management of these 3 complications holds promise for reducing perioperative mortality. Study registration: ClinicalTrials.gov, no. NCT00512109.
© 2019 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Clara Chow received support from the National Health and Medical Research Council of Australia and The Heart Foundation (Australia) for a career development fellowship. Robert Sapsford received nonfinancial support in the form of a research nurse funded by the National Institutes of Health Research, and lecture fees from Eli Lilly, MSD and Novo Nordisk. Denis Xavier received grants from Cadila Pharmaceuticals, Boehringer Ingelheim, Astra Zeneca India, Sanofi Aventis, Pfizer, Bristol–Myers Squibb, Medical Research Council (United Kingdom) and Wellcome Trust outside the submitted work. Emmanuelle Duceppe received a grant as a coapplicant on an investigator-initiated study and lecture fees from Roche Diagnostics. Philip J. Devereaux is a member of a research group with a policy of not accepting honorariums or other payments from industry for their own personal financial gain. They do accept honorariums or payments from industry to support research endeavours and costs to participate in meetings. Based on study questions Dr. Devereaux has originated and grants he has written, he has received grants from Abbott Diagnostics, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers-Squibb, Coviden, Octapharma, Philips Healthcare, Roche Diagnostics, Siemens and Stryker. Dr Devereaux has participated in advisory board meetings for GlaxoSmithKline and Boehringer Ingelheim. He also attended an expert panel meeting with AstraZeneca and Boehringer Ingelheim. Roche Diagnostics provided Troponin T assays and financial support for the Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Study. No other competing interests were declared.
Figures

Comment in
-
Appraising descriptive and analytic findings of large cohort studies.CMAJ. 2019 Jul 29;191(30):E828-E829. doi: 10.1503/cmaj.190882. CMAJ. 2019. PMID: 31809258 Free PMC article. No abstract available.
References
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 2008; 372:139–44. - PubMed
-
- Devereaux PJ, Sessler DI. Cardiac complications in patients undergoing major noncardiac surgery. N Engl J Med 2015;373:2258–69. - PubMed
-
- Botto F, Alonso-Coello P, Chan MT, et al. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014;120:564–78. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical