

Migration rather than proliferation transcriptomic signatures are strongly associated with breast cancer patient survival
- PMID: 31358840
- PMCID: PMC6662662
- DOI: 10.1038/s41598-019-47440-w
Migration rather than proliferation transcriptomic signatures are strongly associated with breast cancer patient survival
Abstract
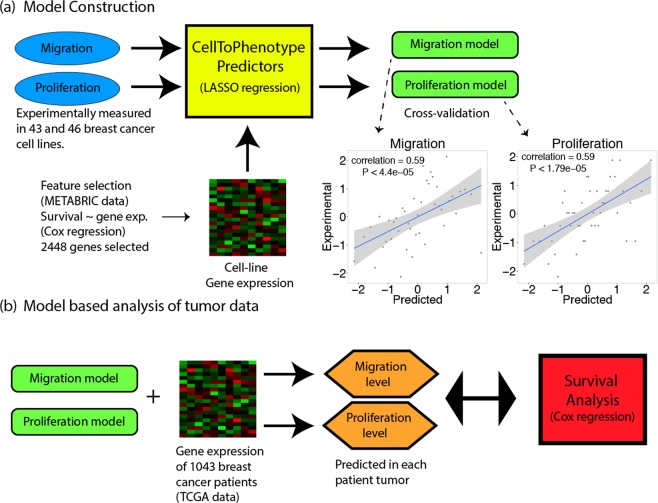
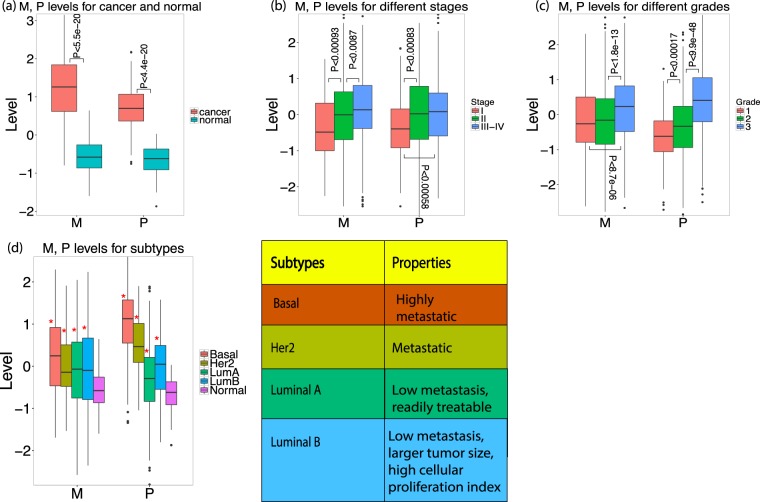
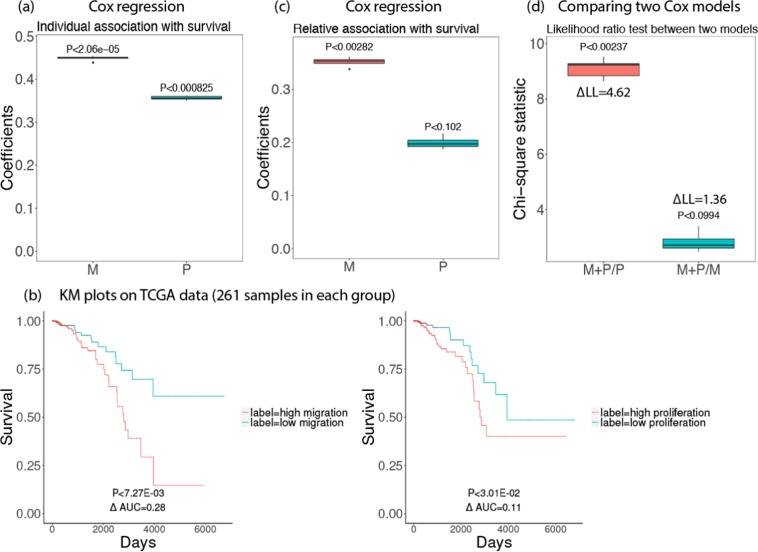
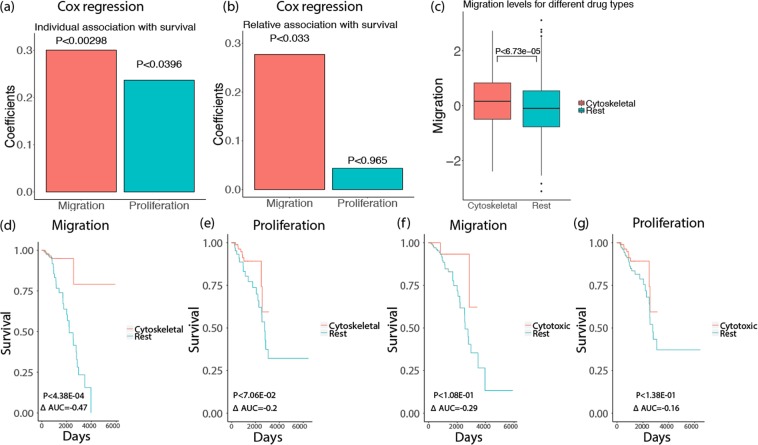
The efficacy of prospective cancer treatments is routinely estimated by in vitro cell-line proliferation screens. However, it is unclear whether tumor aggressiveness and patient survival are influenced more by the proliferative or the migratory properties of cancer cells. To address this question, we experimentally measured proliferation and migration phenotypes across more than 40 breast cancer cell-lines. Based on the latter, we built and validated individual predictors of breast cancer proliferation and migration levels from the cells' transcriptomics. We then apply these predictors to estimate the proliferation and migration levels of more than 1000 TCGA breast cancer tumors. Reassuringly, both estimates increase with tumor's aggressiveness, as qualified by its stage, grade, and subtype. However, predicted tumor migration levels are significantly more strongly associated with patient survival than the proliferation levels. We confirmed these findings by conducting siRNA knock-down experiments on the highly migratory MDA-MB-231 cell lines and deriving gene knock-down based proliferation and migration signatures. We show that cytoskeletal drugs might be more beneficial in patients with high predicted migration levels. Taken together, these results testify to the importance of migration levels in determining patient survival.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Torjesen, I. Drug development: the journey of a medicine from lab to shelf. Pharmaceutical Journal (2015).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
