

Treatment of splenic flexure colon cancer: a comparison of three different surgical procedures: Experience of a high volume cancer center
- PMID: 31358904
- PMCID: PMC6662908
- DOI: 10.1038/s41598-019-47548-z
Treatment of splenic flexure colon cancer: a comparison of three different surgical procedures: Experience of a high volume cancer center
Abstract
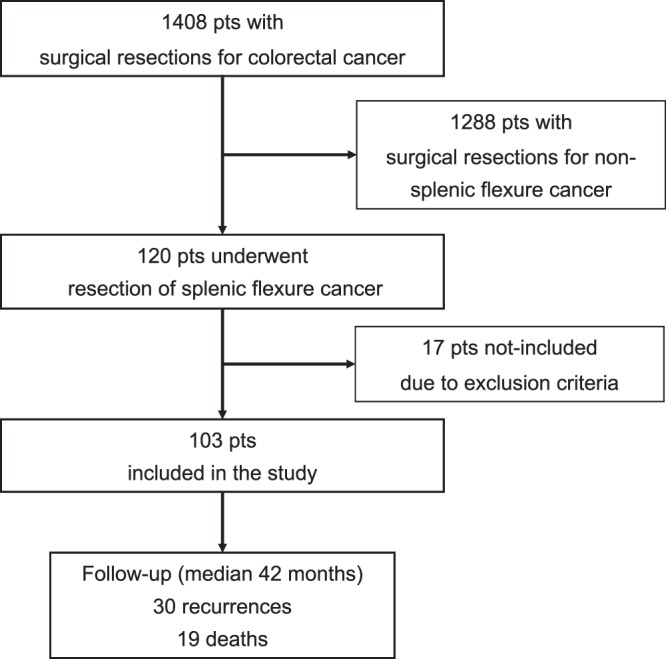
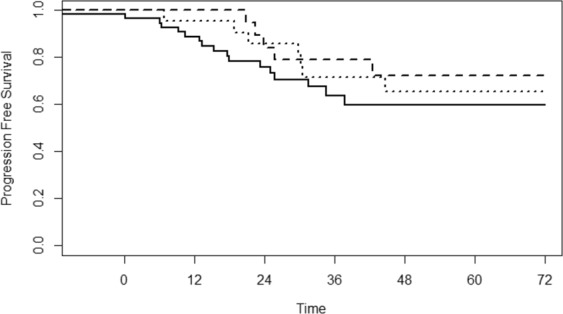
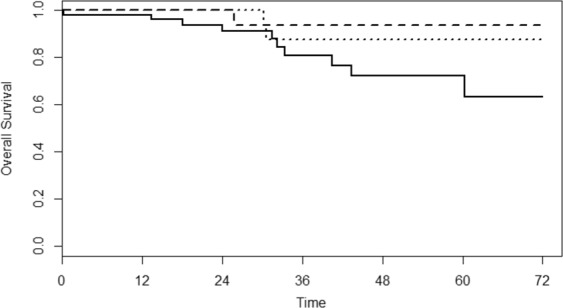
Extended right or left hemicolectomy are the most common surgical treatments for splenic flexure colon cancer. Extended resection (including distal pancreasectomy and/or splenectomy), has been often indicated for the treatment for the splenic flexure cancer, because the lymphatic drainage at this site is poorly defined and assumed as heterogeneous. Between January 2006 and May 2016, 103 patients with splenic flexure colon cancer were enrolled in the study. We evaluated the clinicopathological findings and outcomes of all patients and associated them to the different surgical treatment. Out of 103 selected cases an extended right hemicolectomy was performed in 22 (21.4%) patients, an extended left hemicolectomy in 24 (23.3%) patients, a segmental resection of the splenic flexure in 57 (55.3%) patients; the combined resection of adjacent organs showing tumor adherence was carried out in 11 (10.7%) patients. The tumor infiltrated near organs (T4) in 5 patients. No significant differences in complications were found among the three groups. In all groups no differences were found in the total number of harvested lymphnodes. After a median follow-up of 42 months, 30 recurrences and 19 deaths occurred (12 for tumor progression). There was no difference in overall and progression free survival among the three different surgical treatments. According to our results, the partial resection of splenic flexure was not associated with a worse prognosis and it was leading for a satisfactory oncological outcome. It is our opinion that the extended surgery is seldomly indicated to cure splenic flexure cancer.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
