

Does providing routine liver volume assessment add value when performing CT surveillance in cirrhotic patients?
- PMID: 31359098
- PMCID: PMC6744349
- DOI: 10.1007/s00261-019-02145-6
Does providing routine liver volume assessment add value when performing CT surveillance in cirrhotic patients?
Abstract
Background: The measurement of liver volume (LV) is considered to be an effective prognosticator for postoperative liver failure in patients undergoing hepatectomy. It is unclear whether LV can be used to predict mortality in cirrhotic patients.
Methods: We enrolled 584 consecutive cirrhotic patients who underwent computerized topography (CT) of the abdomen for hepatocellular carcinoma surveillance and 50 age, gender, race, and BMI-matched controls without liver disease. Total LV (TLV), functional LV (FLV), and segmental liver volume (in cm3) were measured from CT imaging. Cirrhotic subjects were followed until death, liver transplantation, or study closure date of July 31, 2016. The survival data were assessed with log-rank statistics and independent predictors of survival were performed using Cox hazards model.
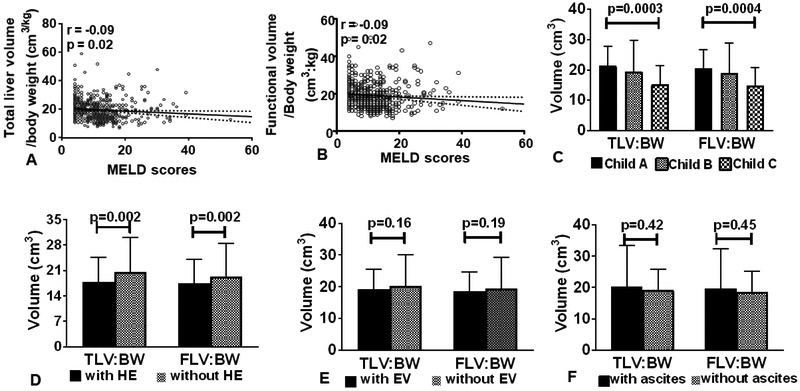
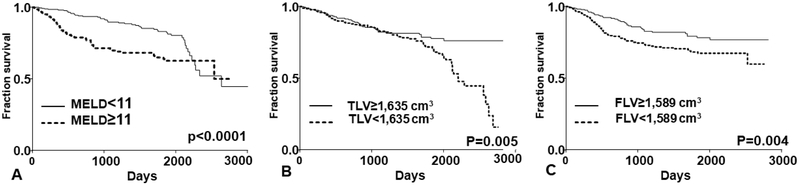
Results: Cirrhotic subjects had significantly lower TLV, FLV, and segmental (all except for segments 1, 6, 7) volume when compared to controls. Subjects presenting with hepatic encephalopathy had significantly lower TLV and FLV than those without HE (p = 0.002). During the median follow-up of 1145 days, 112 (19%) subjects were transplanted and 131 (23%) died. TLV and FLV for those who survived were significantly higher than those who were transplanted or dead (TLV:1740 vs. 1529 vs. 1486, FLV 1691 vs. 1487 vs. 1444, p < 0.0001). In the Cox regression model, age, MELD score, TLV, or FLV were independent predictors of mortality.
Conclusion: Baseline liver volume is an independent predictor of mortality in subjects with cirrhosis. Therefore, it may be useful to provide these data while performing routine surveillance CT scan as an important added value. Further studies are needed to validate these findings and to better understand their clinical utility.
Keywords: Diagnostic imaging; Liver; Portal hypertension.
Conflict of interest statement
Figures
References
-
- Gines P, et al. , Compensated cirrhosis: natural history and prognostic factors. Hepatology, 1987. 7(1): p. 122–128. - PubMed
-
- D’Amico G, Garcia-Tsao G, and Pagliaro L, Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol, 2006. 44(1): p. 217–31. - PubMed
-
- Garcia-Tsao G, Current Management of the Complications of Cirrhosis and Portal Hypertension: Variceal Hemorrhage, Ascites, and Spontaneous Bacterial Peritonitis. Dig Dis, 2016. 34(4): p. 382–6. - PubMed
-
- Garcia-Tsao G, et al. , Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology, 2017. 65(1): p. 310–335. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
