

Female Genital Cutting and Deinfibulation: Applying the Theory of Planned Behavior to Research and Practice
- PMID: 31359211
- PMCID: PMC6987000
- DOI: 10.1007/s10508-019-1427-4
Female Genital Cutting and Deinfibulation: Applying the Theory of Planned Behavior to Research and Practice
Abstract
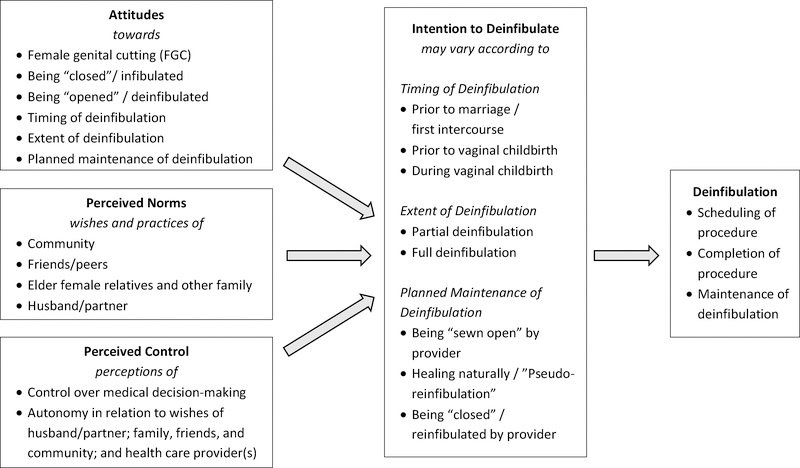
At least 200 million girls and women across the world have experienced female genital cutting (FGC). International migration has grown substantially in recent decades, leading to a need for health care providers in regions of the world that do not practice FGC to become knowledgeable and skilled in their care of women who have undergone the procedure. There are four commonly recognized types of FGC (Types I, II, III, and IV). To adhere to recommendations advanced by the World Health Organization (WHO) and numerous professional organizations, providers should discuss and offer deinfibulation to female patients who have undergone infibulation (Type III FGC), particularly before intercourse and childbirth. Infibulation involves narrowing the vaginal orifice through cutting and appositioning the labia minora and/or labia majora, and creating a covering seal over the vagina with appositioned tissue. The WHO has published a handbook for health care providers that includes guidance in counseling patients about deinfibulation and performing the procedure. Providers may benefit from additional guidance in how to discuss FGC and deinfibulation in a manner that is sensitive to each patient's culture, community, and values. Little research is available to describe decision-making about deinfibulation among women. This article introduces a theoretically informed conceptual model to guide future research and clinical conversations about FGC and deinfibulation with women who have undergone FGC, as well as their partners and families. This conceptual model, based on the Theory of Planned Behavior, may facilitate conversations that lead to shared decision-making between providers and patients.
Keywords: Deinfibulation; Female circumcision; Female genital cutting; Female genital mutilation; Infibulation; Reinfibulation; Shared decision-making; Theory of Planned Behavior.
© 2019. Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Conflict of Interest: The authors declare that they have no conflict of interest.
Figures
Comment in
-
Cutting Cultures: Affective Attachments and Clinical Conundrums.Arch Sex Behav. 2021 Jul;50(5):1959-1962. doi: 10.1007/s10508-019-01614-9. Epub 2020 Jan 2. Arch Sex Behav. 2021. PMID: 31897827 No abstract available.
-
Deinfibulation Contextualized: Delicacies of Shared Decision-Making in the Clinic.Arch Sex Behav. 2021 Jul;50(5):1943-1948. doi: 10.1007/s10508-020-01676-0. Epub 2020 Mar 13. Arch Sex Behav. 2021. PMID: 32170548 Free PMC article. No abstract available.
-
Debating Deinfibulation: Why Some Women Resist the WHO Advice and What Clinicians and Researchers Can Do.Arch Sex Behav. 2021 Jul;50(5):1929-1934. doi: 10.1007/s10508-020-01692-0. Epub 2020 Apr 9. Arch Sex Behav. 2021. PMID: 32274745 No abstract available.
-
Sculptors of African Women's Bodies: Forces Reshaping the Embodiment of Female Genital Cutting in the West.Arch Sex Behav. 2021 Jul;50(5):1949-1957. doi: 10.1007/s10508-020-01710-1. Epub 2020 Apr 23. Arch Sex Behav. 2021. PMID: 32328914 Free PMC article. No abstract available.
-
The Applicability of the Theory of Planned Behavior for Research and Care of Female Genital Cutting.Arch Sex Behav. 2021 Jul;50(5):1935-1941. doi: 10.1007/s10508-020-01716-9. Epub 2020 Apr 26. Arch Sex Behav. 2021. PMID: 32337658 Free PMC article. No abstract available.
-
Response to Commentaries: Applying the Theory of Planned Behavior to Female Genital Cutting and Deinfibulation.Arch Sex Behav. 2021 Jul;50(5):1963-1971. doi: 10.1007/s10508-021-02067-9. Epub 2021 Jun 21. Arch Sex Behav. 2021. PMID: 34155578 Free PMC article. No abstract available.
References
-
- Abdulcadir J, Marras S, Catania L, Abdulcadir O, & Petignat P (In Press). Defibulation: A visual reference and learning tool. The Journal of Sexual Medicine. - PubMed
-
- Ajzen I (1991). The Theory of Planned Behavior. Organizational Behavior and Human Decision Processes, 50, 179–211.
-
- Almroth-Berggren V, Almroth L, Bergström S, Hassanein OM, El Hadi N, & Lithell U (2001). Reinfibulation among women in a rural area in central Sudan. Health Care for Women International, 22, 711–721.
-
- American Academy of Family Physicians. (AAFP). (n.d.). Female genital mutilation. Retrieved from https://www.aafp.org/about/policies/all/genital-mutilation.html
-
- American College of Nurse-Midwives (ACNM). (2017). Position Statement: Female Genital Mutilation/Cutting. Retrieved from http://www.midwife.org/ACNM/files/ACNMLibraryData/UPLOADFILENAME/0000000...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
