

Effect of chronic lymphocytic thyroiditis on the efficacy and safety of ultrasound-guided radiofrequency ablation for papillary thyroid microcarcinoma
- PMID: 31359613
- PMCID: PMC6746112
- DOI: 10.1002/cam4.2406
Effect of chronic lymphocytic thyroiditis on the efficacy and safety of ultrasound-guided radiofrequency ablation for papillary thyroid microcarcinoma
Abstract
Background: Chronic lymphocytic thyroiditis (CLT) is an autoimmune disease commonly associated with papillary thyroid carcinoma characterized by a smaller primary tumor size at presentation. The efficacy and safety of ultrasound-guided radiofrequency ablation (RFA) for papillary thyroid microcarcinoma (PTMC) coexisting with CLT is still unknown.
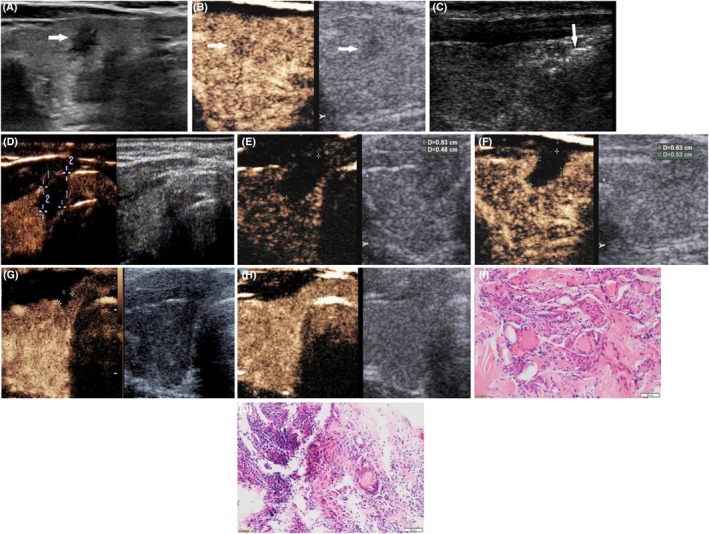
Methods: Sixty patients with unifocal PTMC were enrolled and classified into PTMC and PTMC+CLT groups (n = 30/group). CLT was diagnosed histopathologically. The ablation area exceeded the tumor margins, and was evaluated by US and contrast-enhanced US (CEUS) for residual tumor to prevent recurrence. Three months after ablation, US-guided core-needle biopsy was performed to assess the presence of residual and recurrent cancer. Preoperative and postoperative data on patients and tumors were recorded and analyzed.
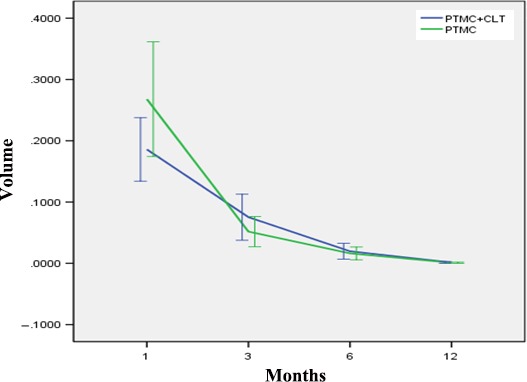
Results: There were no differences between groups in age, sex, preoperative tumor volume, ablation time, or ablation power (P > 0.05). There was also no significant difference in postoperative ablation zone volume between the groups at the 1-, 3-, 6-, 12-, and 18-month follow-ups (P > 0.05). The volume reduction rate significantly differed between the two groups at month 3 (P = 0.03). The ablation area could not be identified on US and CEUS at 9.8 ± 5.0 and 10.0 ± 4.8 months in the PTMC and PTMC + CLT groups, respectively (P = 0.197). No serious complications occurred during and after ablation. No residual cancer cells were found on biopsy after ablation.
Conclusions: RFA was effective in patients with PTMC+CLT, and its therapeutic efficacy and safety were similar to those in patients with PTMC without CLT.
Keywords: ablation; contrast media; radiofrequency; thyroid carcinoma; ultrasonography.
© 2019 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors made no disclosures.
Figures
Similar articles
-
Efficacy and Safety of Ultrasound-Guided Radiofrequency Ablation for Treating Low-Risk Papillary Thyroid Microcarcinoma: A Prospective Study.Thyroid. 2016 Nov;26(11):1581-1587. doi: 10.1089/thy.2015.0471. Epub 2016 Aug 18. Thyroid. 2016. PMID: 27445090
-
Long-term outcomes of radiofrequency ablation for unifocal low-risk papillary thyroid microcarcinoma: a large cohort study of 414 patients.Eur Radiol. 2021 Feb;31(2):685-694. doi: 10.1007/s00330-020-07128-6. Epub 2020 Aug 19. Eur Radiol. 2021. PMID: 32813103
-
Long-Term Follow-Up Results of Ultrasound-Guided Radiofrequency Ablation for Low-Risk Papillary Thyroid Microcarcinoma: More Than 5-Year Follow-Up for 84 Tumors.Thyroid. 2020 Dec;30(12):1745-1751. doi: 10.1089/thy.2020.0106. Epub 2020 Jun 8. Thyroid. 2020. PMID: 32375570
-
Efficacy and safety of ultrasound-guided radiofrequency ablation for papillary thyroid microcarcinoma: a systematic review and meta-analysis.Int J Hyperthermia. 2022;39(1):1300-1309. doi: 10.1080/02656736.2022.2129101. Int J Hyperthermia. 2022. PMID: 36195326
-
Efficacy and safety of radiofrequency, microwave and laser ablation for treating papillary thyroid microcarcinoma: a systematic review and meta-analysis.Int J Hyperthermia. 2019;36(1):1278-1286. doi: 10.1080/02656736.2019.1700559. Int J Hyperthermia. 2019. PMID: 31826684
Cited by
-
Meta-Analysis of the Application Effect of Different Modalities of Thermal Ablation and Surgical Treatment in Papillary Thyroid Microcarcinoma.Dis Markers. 2022 Sep 30;2022:9714140. doi: 10.1155/2022/9714140. eCollection 2022. Dis Markers. 2022. Retraction in: Dis Markers. 2023 Nov 29;2023:9819468. doi: 10.1155/2023/9819468. PMID: 36217504 Free PMC article. Retracted.
-
Five-year follow-up results of thermal ablation for low-risk papillary thyroid microcarcinomas: systematic review and meta-analysis.Eur Radiol. 2021 Sep;31(9):6446-6456. doi: 10.1007/s00330-021-07808-x. Epub 2021 Mar 13. Eur Radiol. 2021. PMID: 33713168
-
Ultrasound-guided microwave ablation for benign thyroid nodules results in earlier and faster nodule shrinkage in patients with Hashimoto's thyroiditis than in those with normal thyroid function.Front Surg. 2023 Jan 26;10:1077077. doi: 10.3389/fsurg.2023.1077077. eCollection 2023. Front Surg. 2023. PMID: 36778645 Free PMC article.
-
[Clinical application of the disposable incision retractor fixator in resection for papillary thyroid carcinoma].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021 Nov;35(11):1028-1030. doi: 10.13201/j.issn.2096-7993.2021.11.014. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2021. PMID: 34886609 Free PMC article. Chinese. No abstract available.
-
Research Review of Thermal Ablation in the Treatment of Papillary Thyroid Carcinoma.Front Oncol. 2022 Jul 1;12:859396. doi: 10.3389/fonc.2022.859396. eCollection 2022. Front Oncol. 2022. PMID: 35847945 Free PMC article. Review.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7‐30. - PubMed
-
- Chen WQ, Li H, Sun KX, et al. Report of cancer incidence and mortality in China, 2014. Zhonghua Zhong Liu Za Zhi. 2018;40:5‐13. - PubMed
-
- Roti E, degli Uberti EC, Bondanelli M, Braverman LE. Thyroid papillary microcarcinoma: a descriptive and meta‐analysis study. Eur J Endocrinol. 2008;159:659‐673. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
