

Alternative iliofemoral revascularization in extensive aortoiliac occlusive disease
- PMID: 31360150
- PMCID: PMC6637000
- DOI: 10.1590/1677-5449.180083
Alternative iliofemoral revascularization in extensive aortoiliac occlusive disease
Abstract
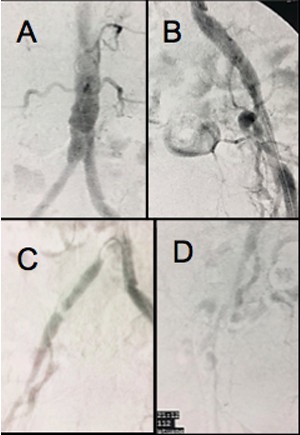
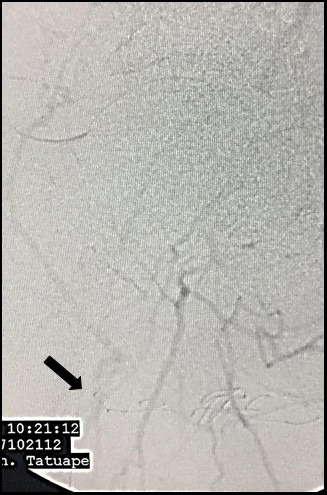
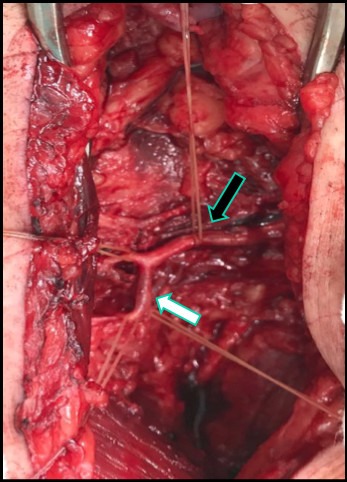
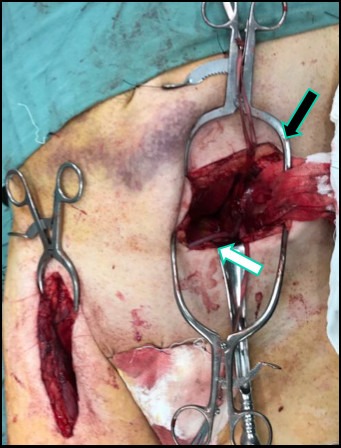
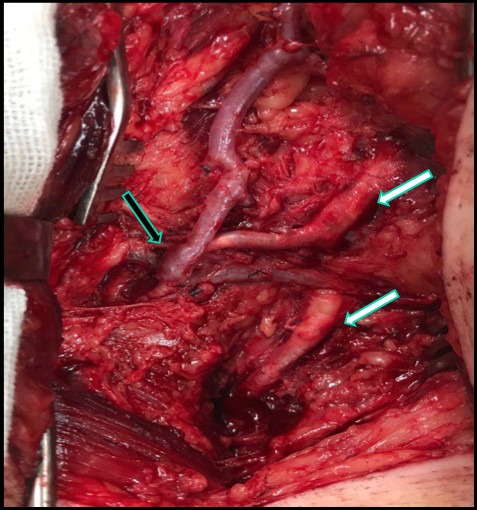
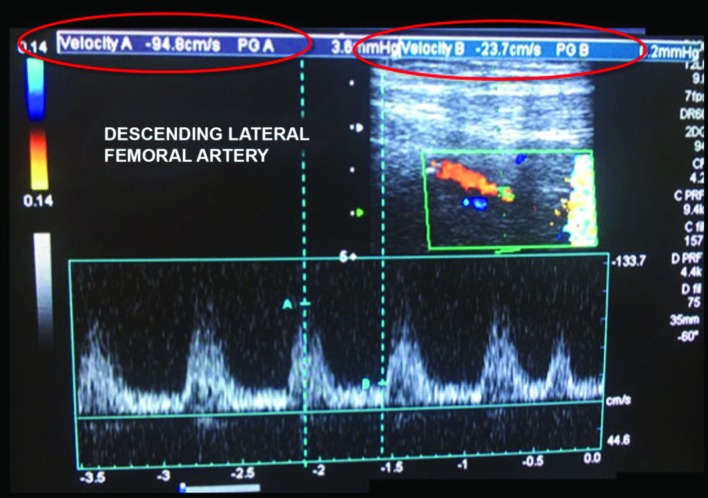
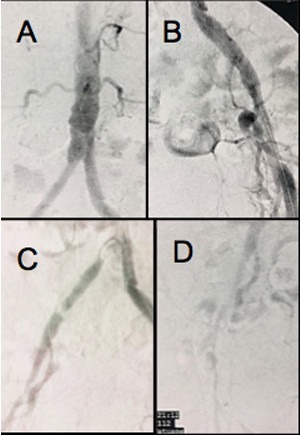
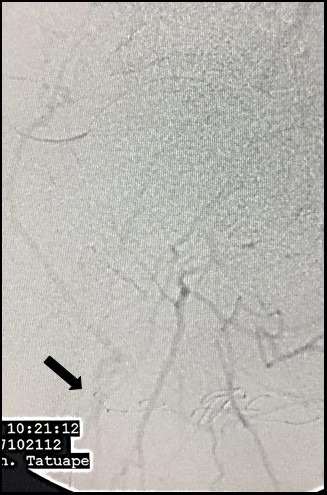
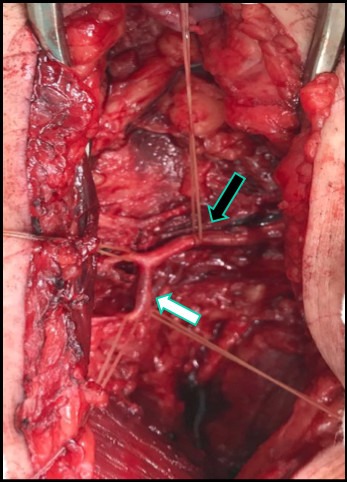
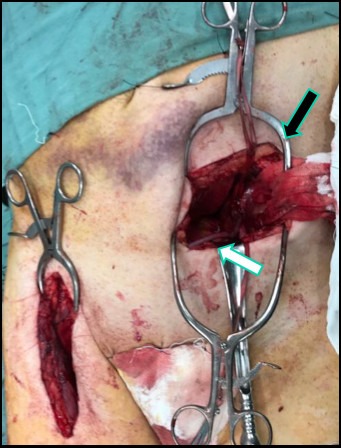
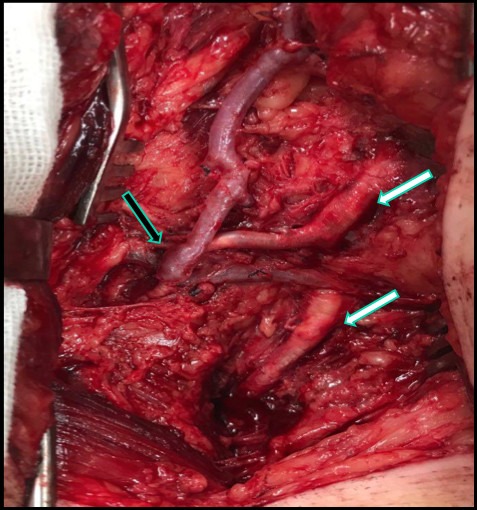
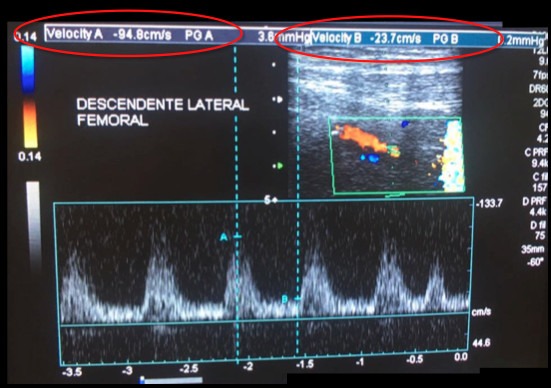
Over recent decades, there has been a considerable increase in use of endovascular methods to treat aortoiliac occlusive disease. It has been demonstrated that this approach offers many benefits, primarily for non-complex arterial lesions of the iliac axis, but difficulties persist with achieving adequate results over the medium and long term when treating extensive occlusive disease. Arterial bypasses to alternative vicarious arteries of the femoral-genicular complex for limb salvage are well known in the literature describing cases that are not favorable for conventional or endovascular surgery. We describe the case of a patient with extensive aortoiliac occlusive disease treated with an arterial bypass in the iliofemoral territory, using an alternative autologous substitute and the descending lateral femoral artery as recipient artery. Alternative bypasses and substitutes that are normally reserved for exceptional cases can and should be part of the vascular therapeutic arsenal and have a contribution to make in cases in which endovascular surgery does not yet enable us to achieve good results.
Resumo: Nas últimas décadas, observou-se o aumento expressivo do tratamento endovascular para a doença oclusiva aortoilíaca. Muitos benefícios foram demonstrados, principalmente nas lesões arteriais não complexas do eixo ilíaco; porém, ainda existe dificuldade na obtenção de resultados adequados a médio e longo prazo quando falamos de doenças oclusivas extensas. As derivações arteriais para artérias vicariantes alternativas do complexo femoro-genicular para salvamento de membro são bem conhecidas na literatura em casos desfavoráveis para cirurgias convencionais ou endovasculares. Descrevemos o caso de um paciente portador de doença oclusiva aortoilíaca extensa tratado com derivação arterial no território ilíaco-femoral, utilizando substituto autógeno alternativo e a artéria descendente femoral lateral como artéria receptora. Derivações e substitutos alternativos, utilizados normalmente em casos de exceção, podem e devem fazer parte do arsenal terapêutico vascular, podendo contribuir nos casos em que a cirurgia endovascular ainda não nos permite alcançar bons resultados.
Keywords: arterial stenosis; atherosclerosis; autologous transplant; vascular graft.
Conflict of interest statement
Conflicts of interest: No conflicts of interest declared concerning the publication of this article.
Figures




Similar articles
-
Descending thoracic aorta to iliofemoral artery bypass grafting: a role for primary revascularization for aortoiliac occlusive disease?J Vasc Surg. 1999 Feb;29(2):249-58. doi: 10.1016/s0741-5214(99)70378-2. J Vasc Surg. 1999. PMID: 9950983
-
Endovascular aortoiliac grafts in combination with standard infrainguinal arterial bypasses in the management of limb-threatening ischemia: preliminary report.J Vasc Surg. 1995 Sep;22(3):316-24; discussion 324-5. doi: 10.1016/s0741-5214(95)70147-8. J Vasc Surg. 1995. PMID: 7674475
-
[Factors determining late patency of aortobifemoral bypass graft].Srp Arh Celok Lek. 1997 Jan-Feb;125(1-2):24-35. Srp Arh Celok Lek. 1997. PMID: 17974352 Serbian.
-
Endovascular grafting for aortoiliac occlusive disease.Semin Vasc Surg. 1997 Dec;10(4):297-309. Semin Vasc Surg. 1997. PMID: 9431600 Review.
-
Clinical application of endovascular grafts in aortoiliac occlusive disease and vascular trauma.Cardiovasc Surg. 1995 Apr;3(2):115-20. doi: 10.1016/0967-2109(95)90883-7. Cardiovasc Surg. 1995. PMID: 7606395 Review.
Cited by
-
Arteriovenous fistula as adjuvant treatment in arterial revascularization of an at-risk limb.J Vasc Bras. 2021 Sep 10;20:e20210042. doi: 10.1590/1677-5449.210042. eCollection 2021. J Vasc Bras. 2021. PMID: 35515087 Free PMC article.
References
LinkOut - more resources
Full Text Sources