

Increased mortality and ICD therapies in ischemic versus non-ischemic dilated cardiomyopathy patients with cardiac resynchronization having survived until first device replacement
- PMID: 31360179
- PMCID: PMC6657262
- DOI: 10.5114/aoms.2018.75139
Increased mortality and ICD therapies in ischemic versus non-ischemic dilated cardiomyopathy patients with cardiac resynchronization having survived until first device replacement
Abstract
Introduction: Cardiac resynchronization therapy combined with an implantable cardioverter defibrillator (CRT-D) is widely applied in heart failure patients. Sufficient data on arrhythmia and defibrillator therapies during long-term follow-up of more than 4 years are lacking and data on mortality are conflicting. We aimed to characterize the occurrence of ventricular arrhythmia, respective defibrillator therapies and mortality for several years following CRT-D implantation or upgrade.
Material and methods: Eighty-eight patients with ischemic (ICM) or non-ischemic dilated cardiomyopathy (DCM) and at least one CRT-D replacement were included in this study and analyzed for incidence of non-sustained ventricular tachycardia (NSVT), defibrillator shocks, anti-tachycardia pacing (ATP) and mortality.
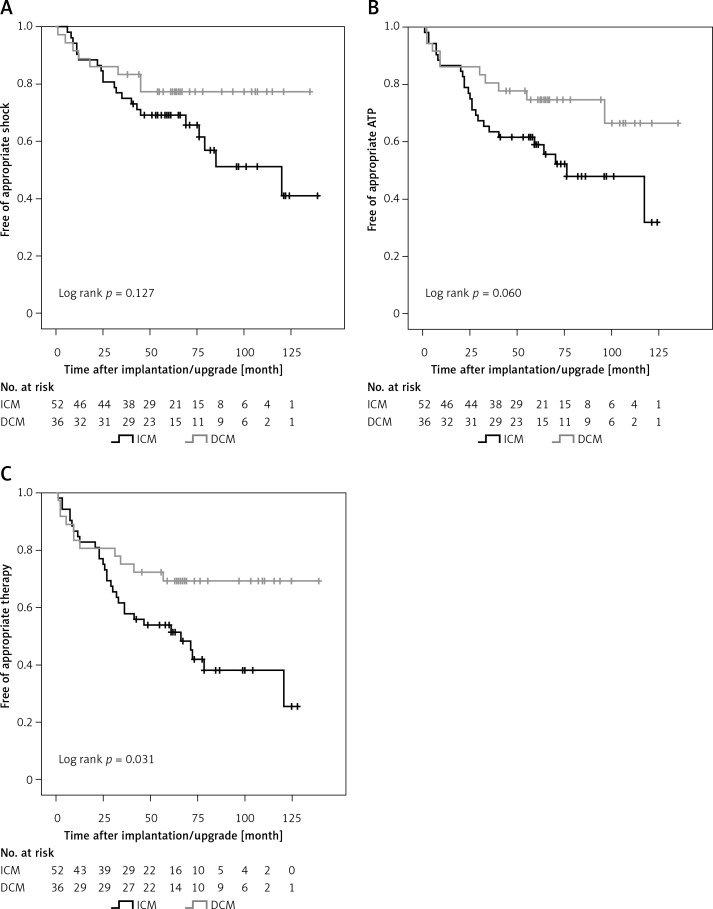
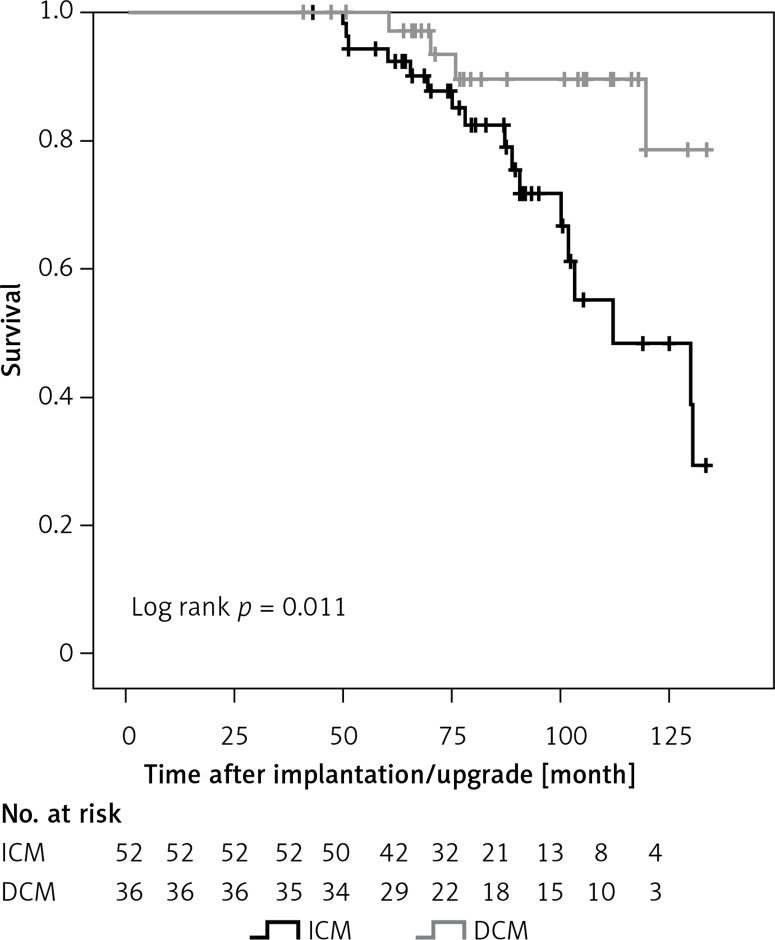
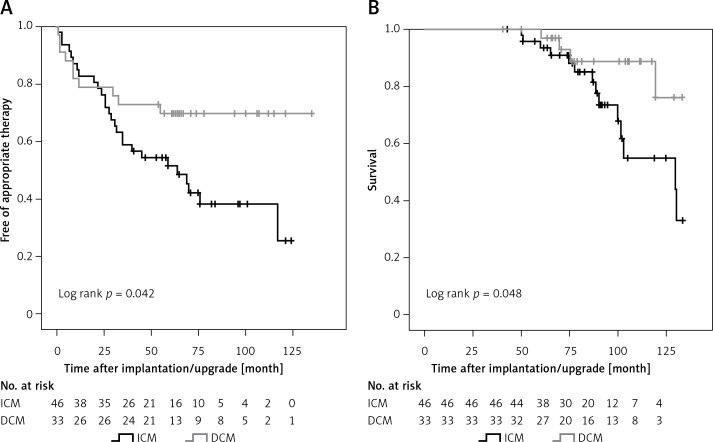
Results: ICM was the underlying disease in 59%, DCM in 41% of patients. During a mean follow-up of 76.4 ±24.8 months the incidence of appropriate defibrillator therapies (shock or ATP) was 46.6% and was elevated in ICM compared to DCM patients (57.7% vs. 30.6%, respectively; p = 0.017). Kaplan-Meier analysis revealed significantly higher ICD therapy-free survival rates in DCM patients (p = 0.031). Left ventricular ejection fraction, NSVT per year and ICM (vs. DCM) were independent predictors of device intervention. The ICM patients showed increased mortality compared to DCM patients, with cumulative all-cause mortality at 9 years of follow-up of 45.4% and 10.6%, respectively. Chronic renal failure, peripheral artery disease and chronic obstructive pulmonary disease were independent predictors of mortality.
Conclusions: The clinical course of patients with ICM and DCM treated with CRT-D differs significantly during long-term follow-up, with increased mortality and incidence of ICD therapies in ICM patients.
Keywords: cardiac resynchronization therapy; heart failure; implantable cardioverter defibrillator; ischemic cardiomyopathy; non-ischemic dilated cardiomyopathy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Tachycardia Therapy Outcomes of Ischemic Versus Nonischemic Cardiomyopathy on Cardiac Resynchronization Therapy: A Propensity Score-matched Analysis.J Community Hosp Intern Med Perspect. 2023 Nov 4;13(6):83-89. doi: 10.55729/2000-9666.1268. eCollection 2023. J Community Hosp Intern Med Perspect. 2023. PMID: 38596550 Free PMC article.
-
Differential outcome of cardiac resynchronization therapy in ischemic cardiomyopathy and idiopathic dilated cardiomyopathy.Heart Rhythm. 2011 Mar;8(3):377-82. doi: 10.1016/j.hrthm.2010.11.013. Epub 2010 Nov 9. Heart Rhythm. 2011. PMID: 21070886
-
Adding Defibrillation Therapy to Cardiac Resynchronization on the Basis of the Myocardial Substrate.J Am Coll Cardiol. 2017 Apr 4;69(13):1669-1678. doi: 10.1016/j.jacc.2017.01.042. J Am Coll Cardiol. 2017. PMID: 28359511
-
Cardiac resynchronization therapy in ischemic and non-ischemic cardiomyopathy.J Arrhythm. 2017 Oct;33(5):410-416. doi: 10.1016/j.joa.2017.03.002. Epub 2017 Apr 21. J Arrhythm. 2017. PMID: 29021842 Free PMC article. Review.
-
Efficacy of Implantable Cardioverter-Defibrillator Therapy in Patients With Nonischemic Cardiomyopathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.JACC Clin Electrophysiol. 2017 Sep;3(9):962-970. doi: 10.1016/j.jacep.2017.02.006. Epub 2017 May 31. JACC Clin Electrophysiol. 2017. PMID: 29759721
Cited by
-
Ischemic Cardiomyopathy versus Non-Ischemic Dilated Cardiomyopathy in Patients with Reduced Ejection Fraction- Clinical Characteristics and Prognosis Depending on Heart Failure Etiology (Data from European Society of Cardiology Heart Failure Registries).Biology (Basel). 2022 Feb 21;11(2):341. doi: 10.3390/biology11020341. Biology (Basel). 2022. PMID: 35205207 Free PMC article.
-
Quantitative Profiling of Serum Carnitines Facilitates the Etiology Diagnosis and Prognosis Prediction in Heart Failure.Molecules. 2023 Jul 11;28(14):5345. doi: 10.3390/molecules28145345. Molecules. 2023. PMID: 37513217 Free PMC article.
-
Prognostic value of lung ultrasonography and bioimpedance spectroscopy in patients with heart failure and reduced ejection fraction.Arch Med Sci. 2020 May 28;20(4):1101-1109. doi: 10.5114/aoms.2020.95727. eCollection 2024. Arch Med Sci. 2020. PMID: 39439690 Free PMC article.
-
One-year outcomes in cardiogenic shock triggered by ventricular arrhythmia: An analysis of the FRENSHOCK multicenter prospective registry.Front Cardiovasc Med. 2023 Jan 26;10:1092904. doi: 10.3389/fcvm.2023.1092904. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 36776263 Free PMC article.
-
Identification of key genes related to heart failure by analysis of expression profiles.Arch Med Sci. 2021 Mar 10;20(2):517-527. doi: 10.5114/aoms/114896. eCollection 2024. Arch Med Sci. 2021. PMID: 38757035 Free PMC article.
References
-
- Brignole M, Auricchio A, Baron-Esquivias G, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA) Eur Heart J. 2013;34:2281–329. - PubMed
-
- Priori SG, Blomstrom-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC) Eur Heart J. 2015;36:2793–867. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Saini A, Kannabhiran M, Reddy P, Gopinathannair R, Olshansky B, Dominic P. Cardiac resynchronization therapy may be antiarrhythmic particularly in responders. JACC Clin Electrophysiol. 2016;2:307–16. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials