

Characterization of T-Cell Receptor Repertoire in Patients with Rheumatoid Arthritis Receiving Biologic Therapies
- PMID: 31360262
- PMCID: PMC6642763
- DOI: 10.1155/2019/2364943
Characterization of T-Cell Receptor Repertoire in Patients with Rheumatoid Arthritis Receiving Biologic Therapies
Abstract
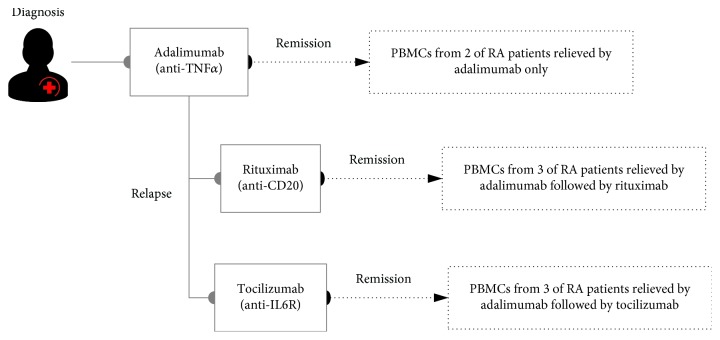
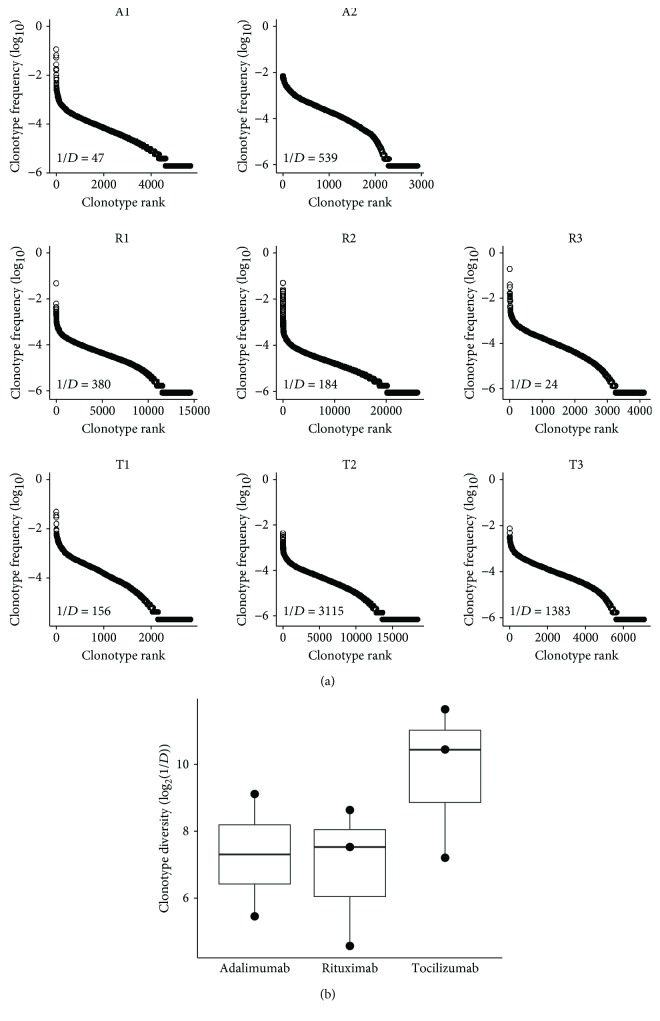
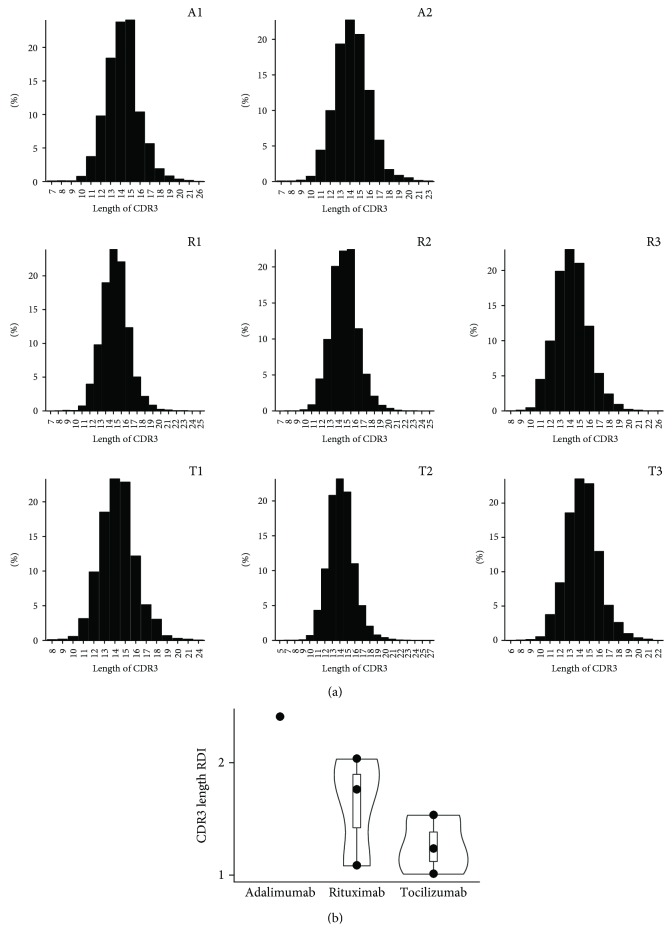
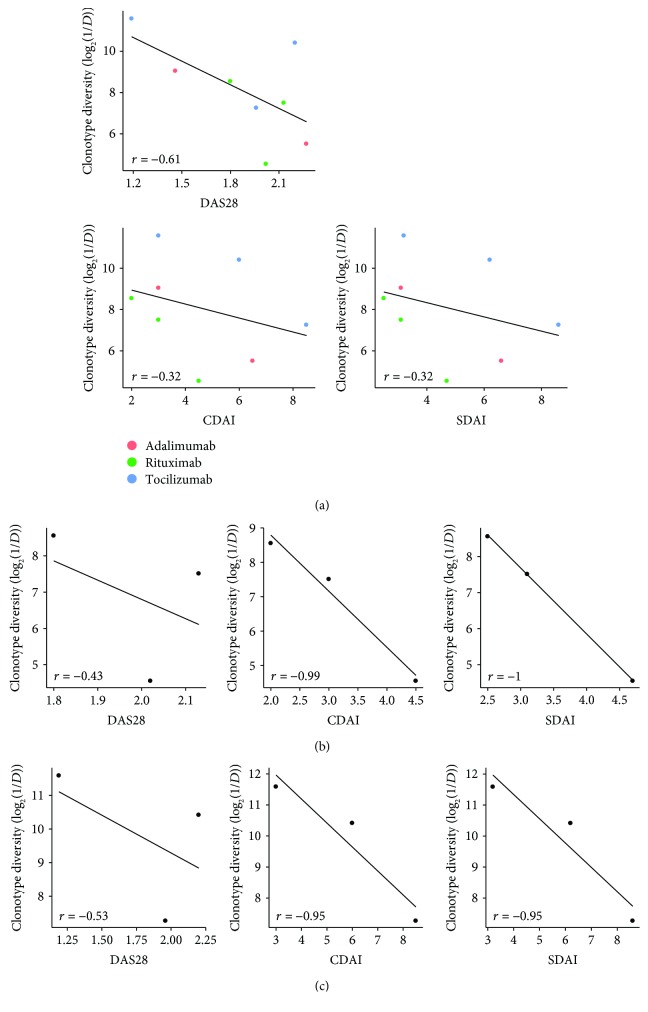
Rheumatoid arthritis (RA) is a systematic autoimmune disease, predominantly causing chronic polyarticular inflammation and joint injury of patients. For the treatment of RA, biologic disease-modifying antirheumatic drugs (bDMARDs) have been used to reduce inflammation and to interfere with disease progression through targeting and mediating the immune system. Although the therapeutic effects of bDMARDs in RA patients have been widely reported, whether these drugs also play important roles in T-cell repertoire status is still unclear. We therefore designed the study to identify the role of T-cell repertoire profiles in RA patients with different types of bDMARD treatments. A high-throughput sequencing approach was applied to profile the T-cell receptor beta chain (TCRB) repertoire of circulating T lymphocytes in eight patients given adalimumab (anti-TNF-α) with/without the following use of either rituximab (anti-CD20) or tocilizumab (anti-IL6R). We subsequently analyzed discrepancies in the clonal diversity and CDR3 length distribution as well as usages of the V and J genes of TCRB repertoire and interrogated the association between repertoire diversity and disease activities followed by the treatment of bDMARDs in these RA patients. All groups of patients showed well-controlled DAS28 scores (<2.6) after different treatment regimens of drugs and displayed no significant statistical differences in repertoire diversity, distribution of CDR3 lengths, and usage of V and J genes of TCRB. Nonetheless, a trend between overall TCRB repertoire diversity and disease activity scores in all bDMARD-treated RA patients was observed. Additionally, age was found to be associated with repertoire diversity in RA patients treated with bDMARDs. Through the profiling of the TCR repertoire in RA patients receiving different biologic medications, our study indicated an inverse tendency between TCR repertoire diversity and disease activity after biologic treatment in RA patients.
Figures

References
-
- Chang W. C., Woon P. Y., Wei J. C., et al. A single-nucleotide polymorphism of CCR6 (rs3093024) is associated with susceptibility to rheumatoid arthritis but not ankylosing spondylitis, in a Taiwanese population. The Journal of Rheumatology. 2012;39(8):1765–1766. doi: 10.3899/jrheum.120040. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
