

Medullary Thyroid Carcinoma: An Update on Imaging
- PMID: 31360432
- PMCID: PMC6642782
- DOI: 10.1155/2019/1893047
Medullary Thyroid Carcinoma: An Update on Imaging
Abstract
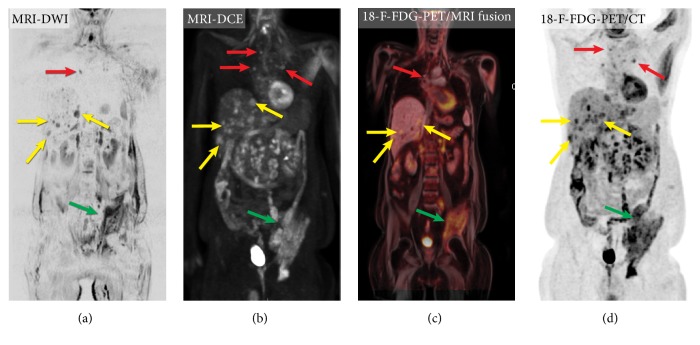
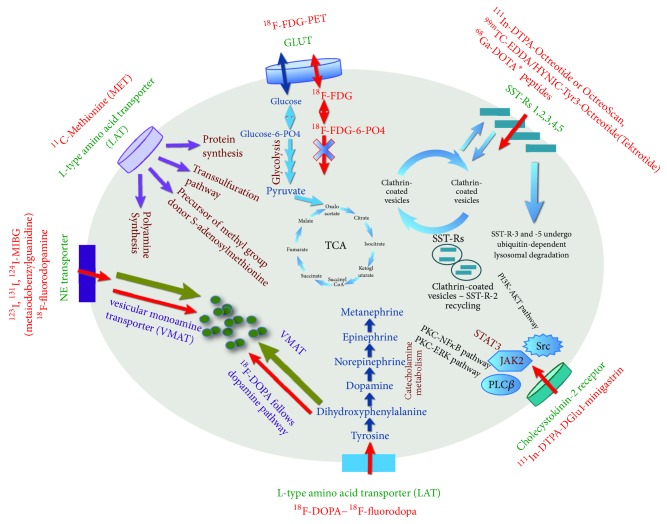
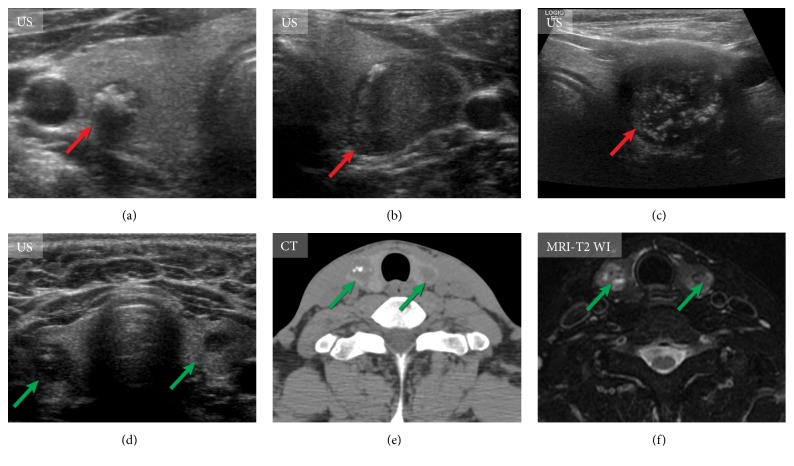
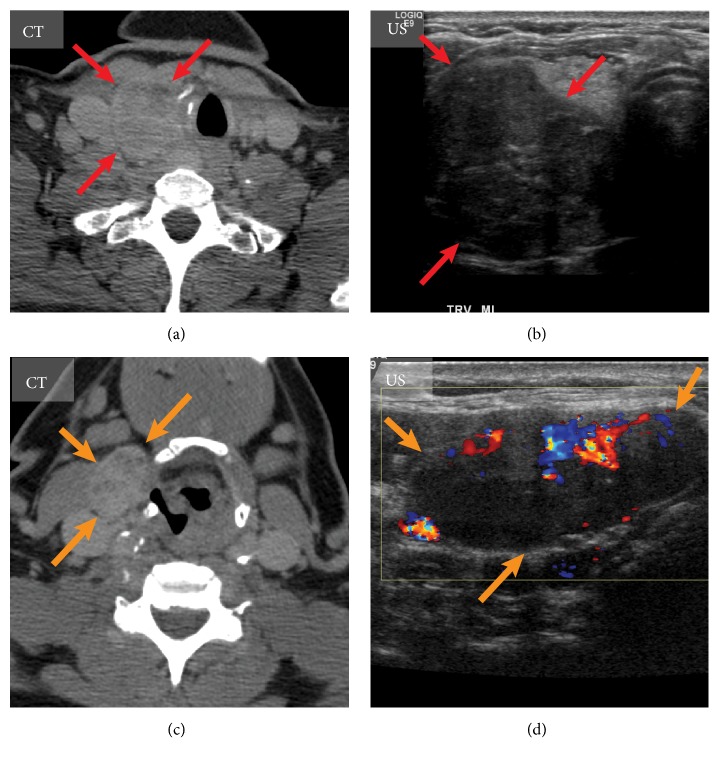
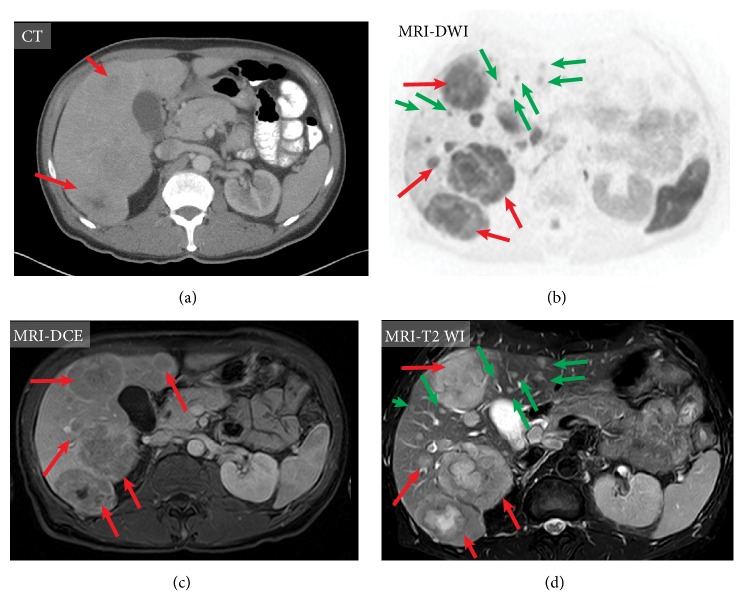
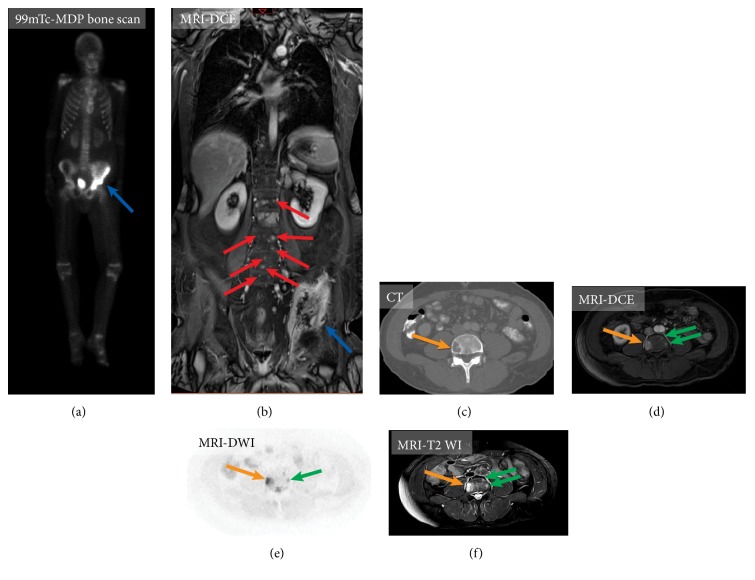
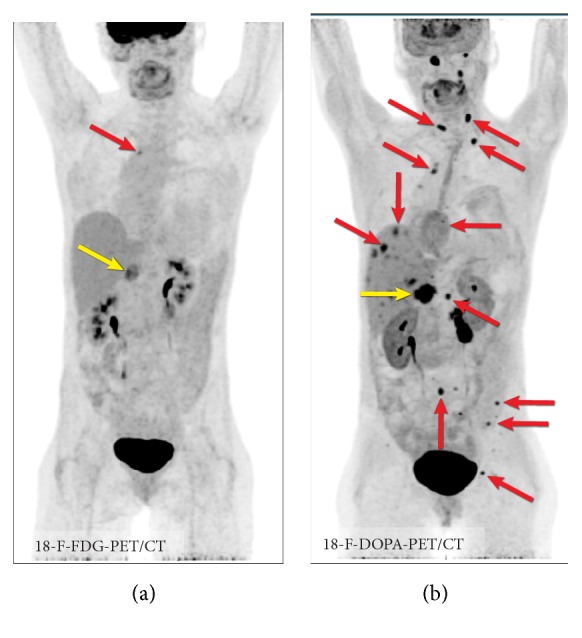
Medullary thyroid carcinoma (MTC), arising from the parafollicular C cells of the thyroid, accounts for 1-2% of thyroid cancers. MTC is frequently aggressive and metastasizes to cervical and mediastinal lymph nodes, lungs, liver, and bones. Although a number of new imaging modalities for directing the management of oncologic patients evolved over the last two decades, the clinical application of these novel techniques is limited in MTC. In this article, we review the biology and molecular aspects of MTC as an important background for the use of current imaging modalities and approaches for this tumor. We discuss the modern and currently available imaging techniques-advanced magnetic resonance imaging (MRI)-based techniques such as whole-body MRI, dynamic contrast-enhanced (DCE) technique, diffusion-weighted imaging (DWI), positron emission tomography/computed tomography (PET/CT) with 18F-FDOPA and 18F-FDG, and integrated positron emission tomography/magnetic resonance (PET/MR) hybrid imaging-for primary as well as metastatic MTC tumor, including its metastatic spread to lymph nodes and the most common sites of distant metastases: lungs, liver, and bones.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
