

The WISDOM Personalized Breast Cancer Screening Trial: Simulation Study to Assess Potential Bias and Analytic Approaches
- PMID: 31360882
- PMCID: PMC6649825
- DOI: 10.1093/jncics/pky067
The WISDOM Personalized Breast Cancer Screening Trial: Simulation Study to Assess Potential Bias and Analytic Approaches
Abstract
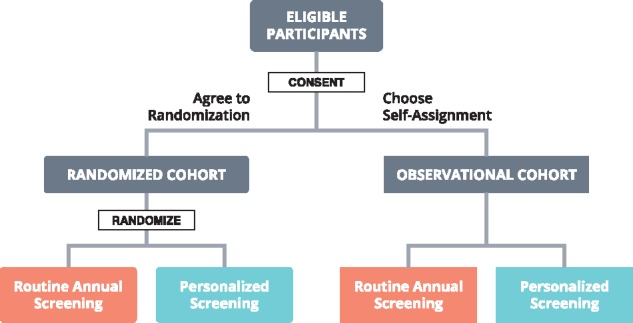
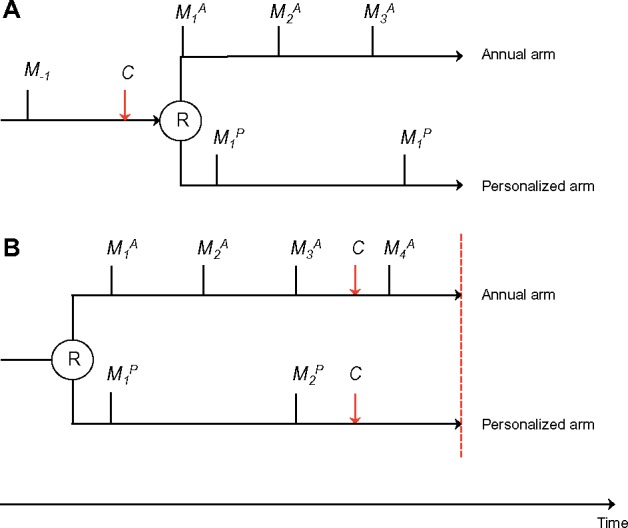
Background: WISDOM (Women Informed to Screen Depending on Measures of Risk) is a randomized trial to assess whether personalized breast cancer screening-where women are screened biannually, annually, biennially, or not at all depending on risk and age-can prevent as many advanced (stage IIB or higher) cancers as annual screening in women ages 40-74 years across 5 years of trial time. The short study time in combination with design choices of not requiring study entry and exit mammograms for all participants may introduce different sources of bias in favor of either the personalized or the annual arm.
Methods: We designed a simulation model and performed 5000 virtual WISDOM trials to assess potential biases. Each virtual trial simulated 65 000 randomly assigned participants who were each assigned a risk stratum and a time to stage of at least IIB cancer sampled from an exponential distribution with the hazard rate based on the risk stratum. Results from the virtual trials were used to evaluate two candidate analysis strategies with respect to susceptibility for introducing bias: 1) difference between arms in total number of events over total trial time, and 2) difference in number of events within complete screening cycles.
Results: Based on the simulations, about 86 stage IIB or higher cancers will be detected within the trial and the total exposure time will be about 74 000 years in each arm. Potential ascertainment bias is introduced at study entry and exit. Analysis strategy 1 works better for the nonscreened stratum, whereas method 2 is considerably more unbiased for the strata of women screened biennially or every 6 months.
Conclusion: Combining the two candidate analysis approaches gives a reasonably unbiased analysis based on the simulations and is the method we will use for the primary analysis in WISDOM. Publishing the WISDOM analysis approach provides transparency and can aid the design and analysis of other individualized screening trials.
Figures
References
-
- Siu AL. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2016;164(4):279–296. - PubMed
-
- Wilt TJ, Harris RP, Qaseem A.. Screening for cancer: advice for high-value care from the American College of Physicians. Ann Intern Med. 2015;162(10):718.. - PubMed
-
- Lee CH, Dershaw DD, Kopans D, et al. Breast cancer screening with imaging: recommendations from the society of breast imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol. 2010;7(1):18–27. - PubMed
-
- Lauby-Secretan B, Scoccianti C, Loomis D, et al. Breast-cancer screening—viewpoint of the IARC working group. N Engl J Med. 2015;372(24):2353–2358. - PubMed