

Factors Contributing to Cancer-Related Muscle Wasting During First-Line Systemic Treatment for Metastatic Colorectal Cancer
- PMID: 31360897
- PMCID: PMC6649832
- DOI: 10.1093/jncics/pkz016
Factors Contributing to Cancer-Related Muscle Wasting During First-Line Systemic Treatment for Metastatic Colorectal Cancer
Abstract
Background: Increasing evidence indicates that loss of muscle mass is associated with adverse outcomes in metastatic colorectal cancer. Here, we investigate which demographic, lifestyle- (smoking), tumor-, and treatment-related factors are associated with muscle loss in patients with metastatic colorectal cancer during first-line palliative systemic treatment.
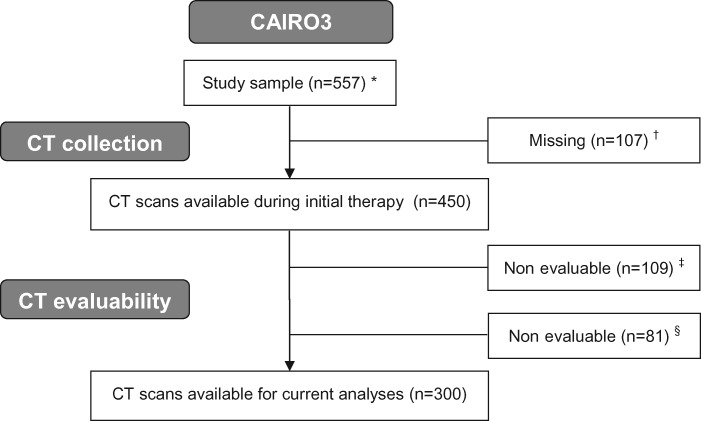
Methods: Data from 300 patients with computed tomography scans both at start and after six initial cycles of capecitabine plus oxaliplatin and bevacizumab was used (CAIRO3). From computed tomography, muscle mass normalized for stature (skeletal muscle index [SMI]) was calculated. A priori-selected variables were tested using multivariable linear regression models (P values ≤.05). Two models were developed: Model 1 contained variables measured at start and Model 2 contained variables assessed after initial therapy.
Results: In Model 1, loss of SMI was statistically significantly associated with a higher initial SMI (-0.32%, 95% confidence interval [CI] = -0.45% to -0.19% per unit increase in initial SMI), smoking status (-2.74%, 95% CI = -5.29% to -0.19% for smokers), and interval of metastases (-3.02%, 95% CI = -5.50% to -0.53%) for metachronous vs synchronous metastases), and primary tumor resection was statistically significantly associated with a gain in SMI (2.17%, 95% CI = 0.13% to 4.21% for resection vs no resection). In Model 2, loss of SMI was statistically significantly associated with response to capecitabine plus oxaliplatin and bevacizumab (-2.48%, 95% CI = -4.33% to -0.62% for stable disease vs partial/complete response).
Conclusions: Our results highlight, given the association of sarcopenia and survival, that patients with higher SMI should not be ignored. In addition, smoking is a potentially modifiable factor associated with muscle loss. The association between smoking and muscle loss might relate to worse clinical outcomes in smokers with metastatic colorectal cancer.
Figures
References
-
- Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol. 2011;12(5):489–495. - PubMed
-
- Bozzetti F. Forcing the vicious circle: sarcopenia increases toxicity, decreases response to chemotherapy and worsens with chemotherapy. Ann Oncol. 2017;28(9):2107–2118. - PubMed
-
- Malietzis G, Aziz O, Bagnall NM, et al. The role of body composition evaluation by computerized tomography in determining colorectal cancer treatment outcomes: a systematic review. Eur J Surg Oncol. 2015;41(2):186–196. - PubMed
-
- Kurk S, Peeters P, Stellato R, et al. Impact of sarcopenia on dose limiting toxicities in metastatic colorectal cancer patients (mCRC pts) receiving palliative systemic treatment. Ann Oncol. 2017;28(suppl 5):544–545.
LinkOut - more resources
Full Text Sources