

A pilot study of prostate-specific membrane antigen (PSMA) dynamics in men undergoing treatment for advanced prostate cancer
- PMID: 31361358
- PMCID: PMC6818502
- DOI: 10.1002/pros.23883
A pilot study of prostate-specific membrane antigen (PSMA) dynamics in men undergoing treatment for advanced prostate cancer
Abstract
Background: Prostate-specific membrane antigen (PSMA) is a rational target for noninvasive detection of recurrent prostate cancer (PCa) and for therapy of metastatic castration-resistant prostate cancer (mCRPC) with PSMA-targeted agents. Here we conducted serial measurements of PSMA expression on circulating tumor cells (CTCs) to evaluate patterns of longitudinal PSMA dynamics over the course of multiple sequential therapies.
Methods: A retrospective investigation of men with mCRPC undergoing evaluation at medical oncology clinics at our institution assessed the dynamics of PSMA expression in the context of different systemic treatments administered sequentially. Eligibility included patients who began systemic therapies with androgen receptor (AR)-directed agents or taxane agents for whom peripheral blood samples were tested for CTC mRNA of AR splice variant-7 (AR-V7), prostate-specific antigen (PSA), and PSMA (with >2 CTC + results) in a CLIA-accredited laboratory.
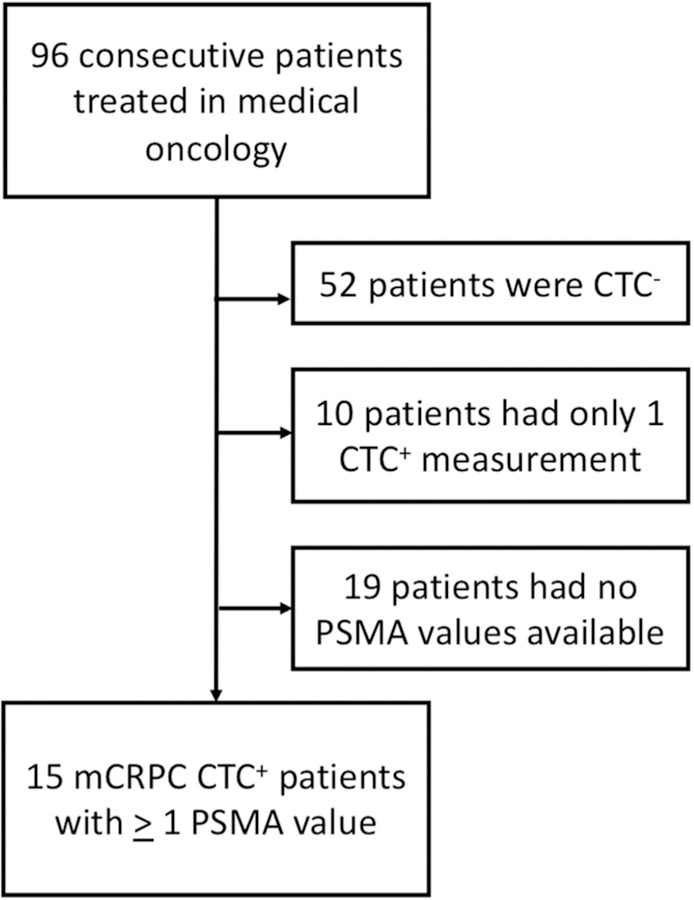
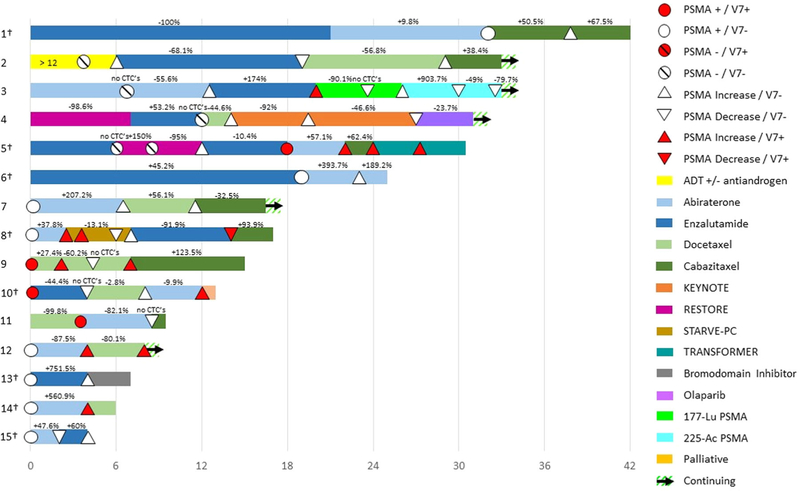
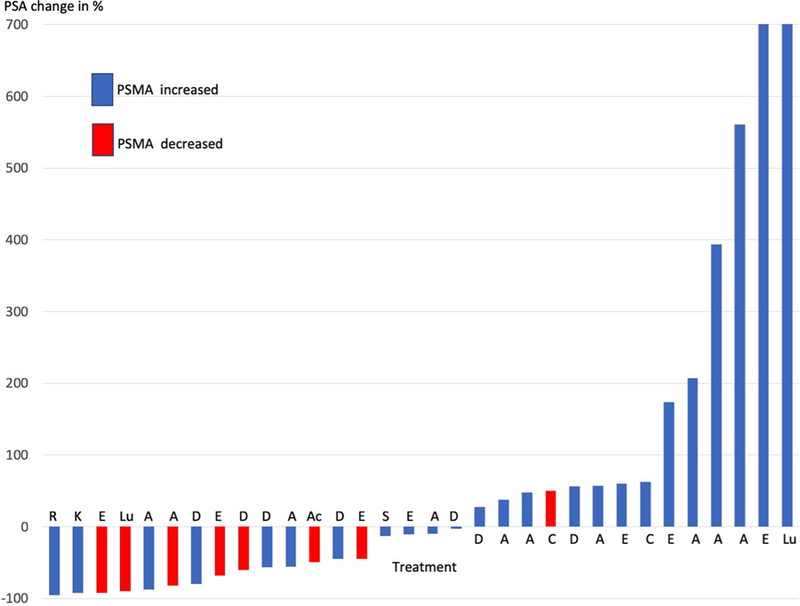
Results: From August 2015 to November 2017, we identified 96 eligible men. Fifteen had greater than or equal to 2 sequential therapies and evaluable CTC samples, greater than or equal to 1 expressing PSMA (PSMA+). Among the 15 patients included in this analysis, a total of 54 PSMA status evaluations were performed in the context of 48 therapies during a median follow-up of 18 months. At baseline, PSMA signal was detected ("positive") in 11 of 15 (73.3%) patients, while for 4 of 15 (26.7%) patients PSMA signal was undetectable ("negative"). In all but two patients, the baseline collection corresponded with a change in treatment. On the second assessment, PSMA increases were detected in all 4/4 (100%) PSMA-negative patients and 8 of 11 (72.7%) PSMA-positive patients. PSMA significantly decreased in a patient treated with 177 Lu-PSMA-617. Serum PSA declines were seen in 7 of 8 (88%) of the treatment periods where PSMA decreased.
Conclusions: PSMA expression in CTCs is a dynamic marker. PSMA transcript declines appear to be associated with concurrent decreases in serum PSA. Sequential CTC sampling could provide a noninvasive response assessment to systemic treatment for mCRPC.
Keywords: PSA; PSMA; circulating tumor cells; metastatic prostate cancer; prostate-specific membrane antigen.
© 2019 Wiley Periodicals, Inc.
Conflict of interest statement
CONFLICT OF INTERESTS
Remaining authors declare that there are no conflict of interests.
Figures
Similar articles
-
Molecular analysis of circulating tumor cells of metastatic castration-resistant Prostate Cancer Patients receiving 177Lu-PSMA-617 Radioligand Therapy.Theranostics. 2020 Jun 18;10(17):7645-7655. doi: 10.7150/thno.44556. eCollection 2020. Theranostics. 2020. PMID: 32685010 Free PMC article.
-
[177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial.Lancet. 2021 Feb 27;397(10276):797-804. doi: 10.1016/S0140-6736(21)00237-3. Epub 2021 Feb 11. Lancet. 2021. PMID: 33581798 Clinical Trial.
-
Impact of Circulating Tumor Cell-Expressed Prostate-Specific Membrane Antigen and Prostate-Specific Antigen Transcripts in Different Stages of Prostate Cancer.Clin Cancer Res. 2024 May 1;30(9):1788-1800. doi: 10.1158/1078-0432.CCR-23-3083. Clin Cancer Res. 2024. PMID: 38587547
-
Efficacy Against Human Prostate Cancer by Prostate-specific Membrane Antigen-specific, Transforming Growth Factor-β Insensitive Genetically Targeted CD8+ T-cells Derived from Patients with Metastatic Castrate-resistant Disease.Eur Urol. 2018 May;73(5):648-652. doi: 10.1016/j.eururo.2017.12.008. Epub 2017 Dec 21. Eur Urol. 2018. PMID: 29275833 Free PMC article. Review.
-
[PSMA-targeted radioligand therapy in prostate cancer].Urologe A. 2017 Jan;56(1):32-39. doi: 10.1007/s00120-016-0274-3. Urologe A. 2017. PMID: 27885457 Review. German.
Cited by
-
Bridging the Gaps between Circulating Tumor Cells and DNA Methylation in Prostate Cancer.Cancers (Basel). 2021 Aug 21;13(16):4209. doi: 10.3390/cancers13164209. Cancers (Basel). 2021. PMID: 34439363 Free PMC article. Review.
-
Advanced single-cell and spatial analysis with high-multiplex characterization of circulating tumor cells and tumor tissue in prostate cancer: Unveiling resistance mechanisms with the CoDuCo in situ assay.Biomark Res. 2024 Nov 16;12(1):140. doi: 10.1186/s40364-024-00680-z. Biomark Res. 2024. PMID: 39550585 Free PMC article.
-
PROTAC technology for prostate cancer treatment.Acta Mater Med. 2025 Jan 7;4(1):99-121. doi: 10.15212/amm-2024-0075. Epub 2025 Jan 30. Acta Mater Med. 2025. PMID: 40832004 Free PMC article.
-
Detecting androgen receptor (AR), AR variant 7 (AR-V7), prostate-specific membrane antigen (PSMA), and prostate-specific antigen (PSA) gene expression in CTCs and plasma exosome-derived cfRNA in patients with metastatic castration-resistant prostate cancer (mCRPC) by integrating the VTX-1 CTC isolation system with the QIAGEN AdnaTest.BMC Cancer. 2024 Apr 16;24(1):482. doi: 10.1186/s12885-024-12139-3. BMC Cancer. 2024. PMID: 38627648 Free PMC article.
-
Integrated Therapeutic Targeting of the Prostate Tumor Microenvironment.Adv Exp Med Biol. 2020;1296:183-198. doi: 10.1007/978-3-030-59038-3_11. Adv Exp Med Biol. 2020. PMID: 34185293
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. - PubMed
-
- Rowe SP, Gorin MA, Pomper MG. Imaging of prostate-specific membrane antigen with small-molecule pet radiotracers: from the bench to advanced clinical applications. Annu Rev Med. 2019;70: 461–477. - PubMed
-
- Sweat SD, Pacelli A, Murphy GP, Bostwick DG. Prostate-specific membrane antigen expression is greatest in prostate adenocarcinoma and lymph node metastases. Urology. 1998;52(4):637–640. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
