

Crystal deposition triggers tubule dilation that accelerates cystogenesis in polycystic kidney disease
- PMID: 31361604
- PMCID: PMC6763267
- DOI: 10.1172/JCI128503
Crystal deposition triggers tubule dilation that accelerates cystogenesis in polycystic kidney disease
Abstract
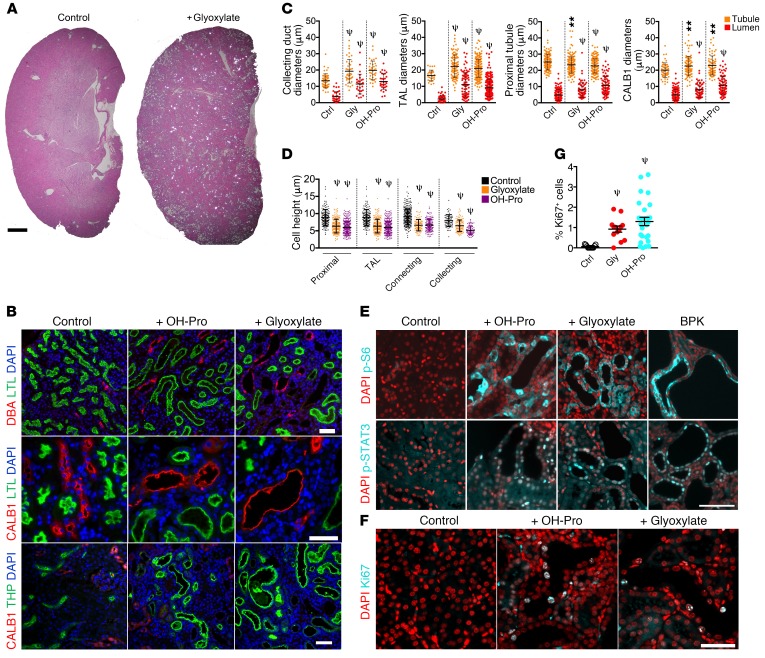
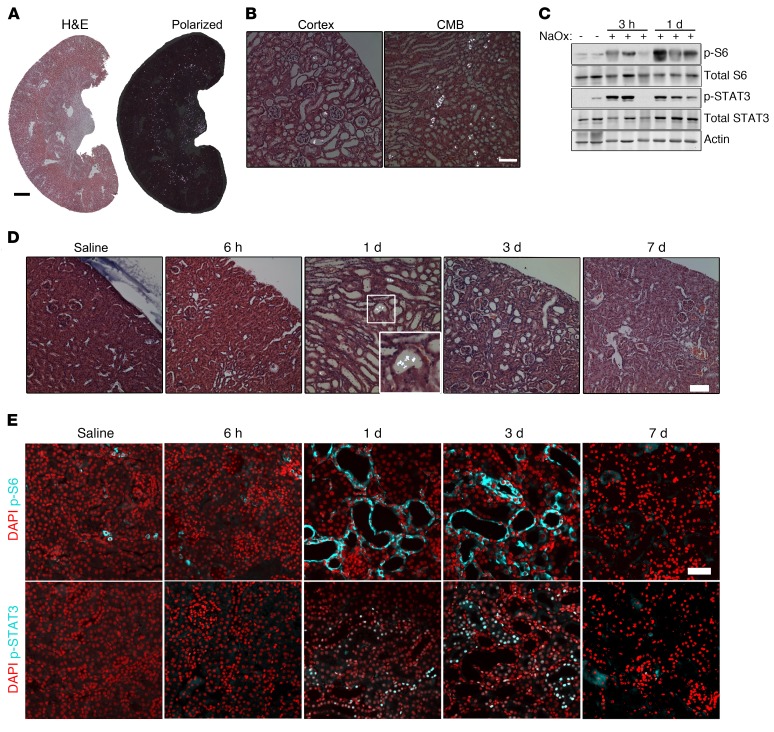
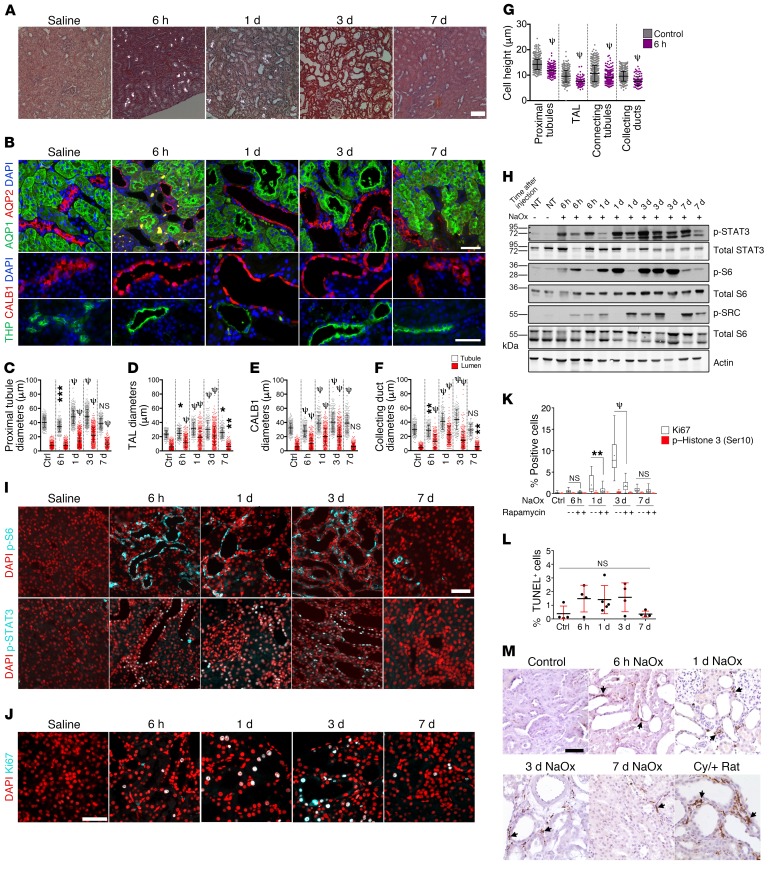
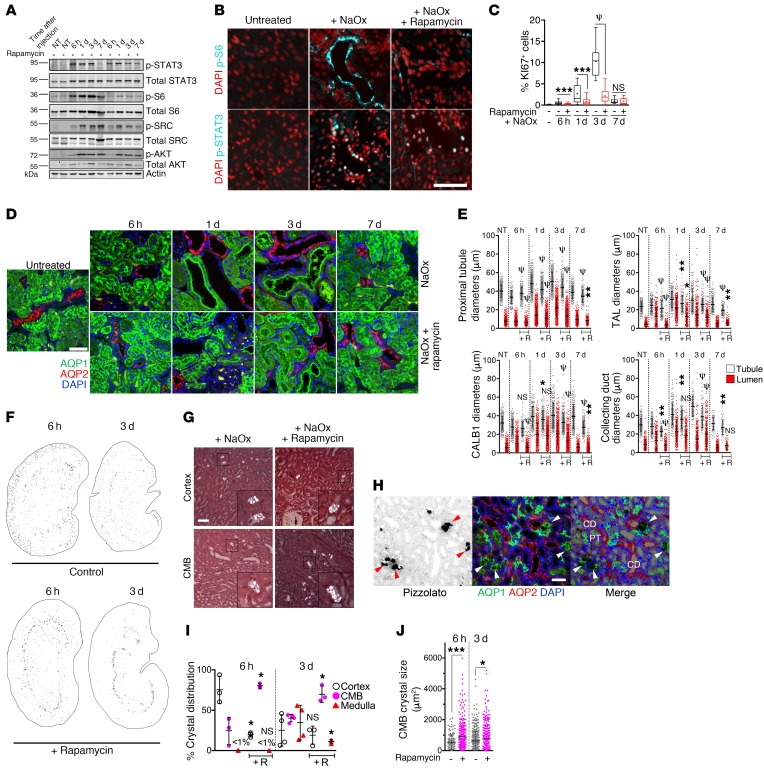
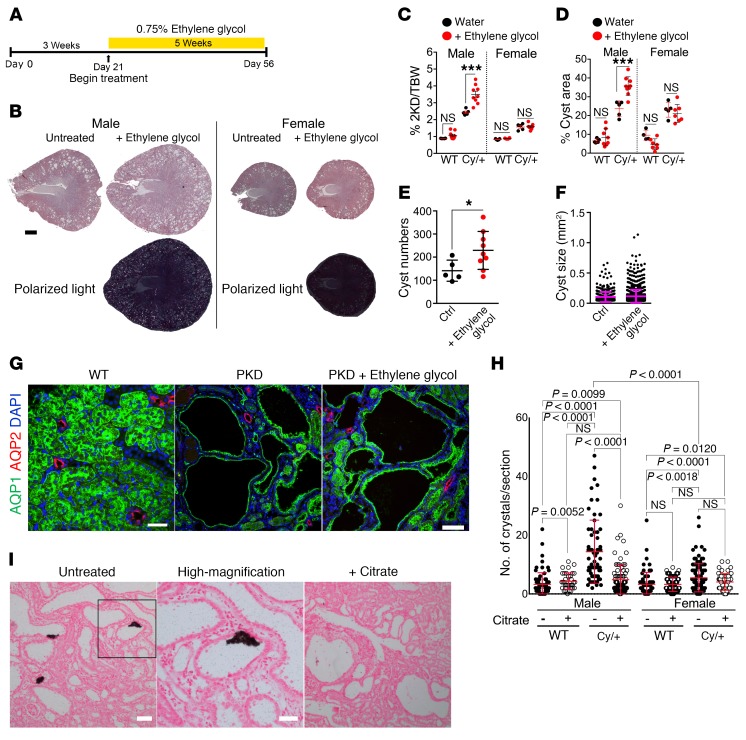
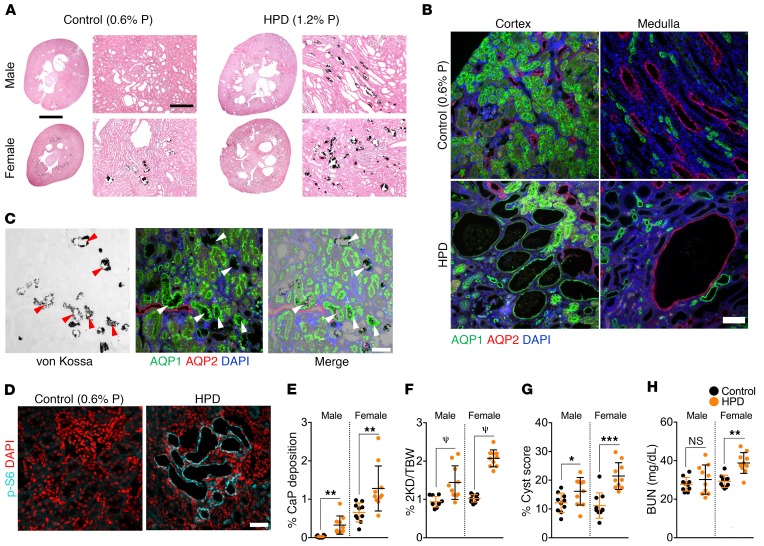
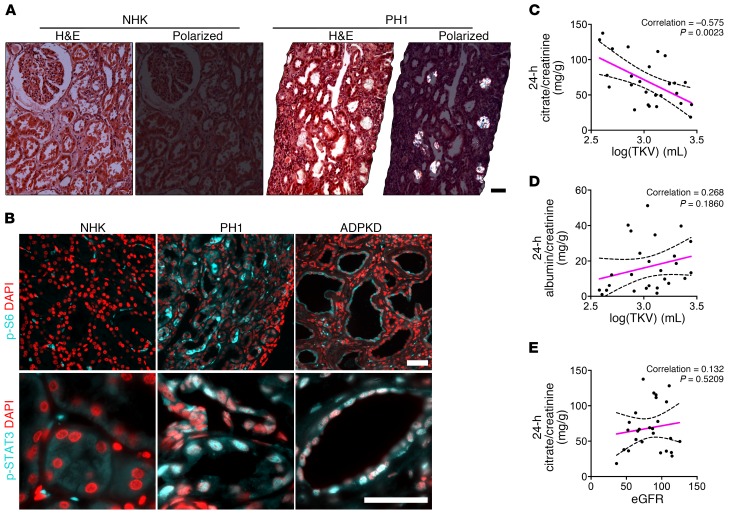
The rate of disease progression in autosomal-dominant (AD) polycystic kidney disease (PKD) exhibits high intra-familial variability suggesting that environmental factors may play a role. We hypothesized that a prevalent form of renal insult may accelerate cystic progression and investigated tubular crystal deposition. We report that calcium oxalate (CaOx) crystal deposition led to rapid tubule dilation, activation of PKD-associated signaling pathways, and hypertrophy in tubule segments along the affected nephrons. Blocking mTOR signaling blunted this response and inhibited efficient excretion of lodged crystals. This mechanism of "flushing out" crystals by purposefully dilating renal tubules has not previously been recognized. Challenging PKD rat models with CaOx crystal deposition, or inducing calcium phosphate deposition by increasing dietary phosphorous intake, led to increased cystogenesis and disease progression. In a cohort of ADPKD patients, lower levels of urinary excretion of citrate, an endogenous inhibitor of calcium crystal formation, correlated with increased disease severity. These results suggest that PKD progression may be accelerated by commonly occurring renal crystal deposition which could be therapeutically controlled by relatively simple measures.
Keywords: Fibrosis; Genetic diseases; Nephrology.
Conflict of interest statement
Figures
Comment in
-
Crystal deposition aids cystogenesis.Nat Rev Nephrol. 2019 Dec;15(12):730. doi: 10.1038/s41581-019-0215-7. Nat Rev Nephrol. 2019. PMID: 31551591 No abstract available.
Similar articles
-
Potential role of fluctuations in the composition of renal tubular fluid through the nephron in the initiation of Randall's plugs and calcium oxalate crystalluria in a computer model of renal function.Urolithiasis. 2015 Jan;43 Suppl 1:93-107. doi: 10.1007/s00240-014-0737-1. Epub 2014 Nov 20. Urolithiasis. 2015. PMID: 25407799
-
Urinary Citrate Is Associated with Kidney Outcomes in Early Polycystic Kidney Disease.Kidney360. 2022 Oct 17;3(12):2110-2115. doi: 10.34067/KID.0004772022. eCollection 2022 Dec 29. Kidney360. 2022. PMID: 36591350 Free PMC article.
-
[Effect of a modified low protein and low fat diet on histologic changes and metabolism in kidneys in an experimental model of polycystic kidney disease].Srp Arh Celok Lek. 2002 Jul-Aug;130(7-8):251-7. Srp Arh Celok Lek. 2002. PMID: 12585002 Serbian.
-
Kidney models of calcium oxalate stone formation.Nephron Physiol. 2004;98(2):p21-30. doi: 10.1159/000080260. Nephron Physiol. 2004. PMID: 15499211 Review.
-
Nephrolithiasis: a consequence of renal epithelial cell exposure to oxalate and calcium oxalate crystals.Mol Urol. 2000 Winter;4(4):305-12. Mol Urol. 2000. PMID: 11156696 Review.
Cited by
-
Metabolism-based approaches for autosomal dominant polycystic kidney disease.Front Mol Biosci. 2023 Feb 16;10:1126055. doi: 10.3389/fmolb.2023.1126055. eCollection 2023. Front Mol Biosci. 2023. PMID: 36876046 Free PMC article. Review.
-
STAT signaling in polycystic kidney disease.Cell Signal. 2020 Aug;72:109639. doi: 10.1016/j.cellsig.2020.109639. Epub 2020 Apr 20. Cell Signal. 2020. PMID: 32325185 Free PMC article. Review.
-
Polycystic Kidney Disease Diet: What is Known and What is Safe.Clin J Am Soc Nephrol. 2024 May 1;19(5):664-682. doi: 10.2215/CJN.0000000000000326. Epub 2023 Sep 20. Clin J Am Soc Nephrol. 2024. PMID: 37729939 Free PMC article. Review.
-
Kidney stone formation in a novel murine model of polycystic kidney disease.Am J Physiol Renal Physiol. 2022 Jul 1;323(1):F59-F68. doi: 10.1152/ajprenal.00165.2021. Epub 2022 Mar 28. Am J Physiol Renal Physiol. 2022. PMID: 35343849 Free PMC article.
-
Review of the Use of Animal Models of Human Polycystic Kidney Disease for the Evaluation of Experimental Therapeutic Modalities.J Clin Med. 2023 Jan 14;12(2):668. doi: 10.3390/jcm12020668. J Clin Med. 2023. PMID: 36675597 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
