

Health checks and cardiovascular risk factor values over six years' follow-up: Matched cohort study using electronic health records in England
- PMID: 31361740
- PMCID: PMC6667114
- DOI: 10.1371/journal.pmed.1002863
Health checks and cardiovascular risk factor values over six years' follow-up: Matched cohort study using electronic health records in England
Abstract
Background: The National Health Service (NHS) in England introduced a population-wide programme for cardiovascular disease (CVD) prevention in 2009, known as NHS Health Checks. This research aimed to measure the cardiovascular risk management and cardiovascular risk factor outcomes of the health check programme during six years' follow-up.
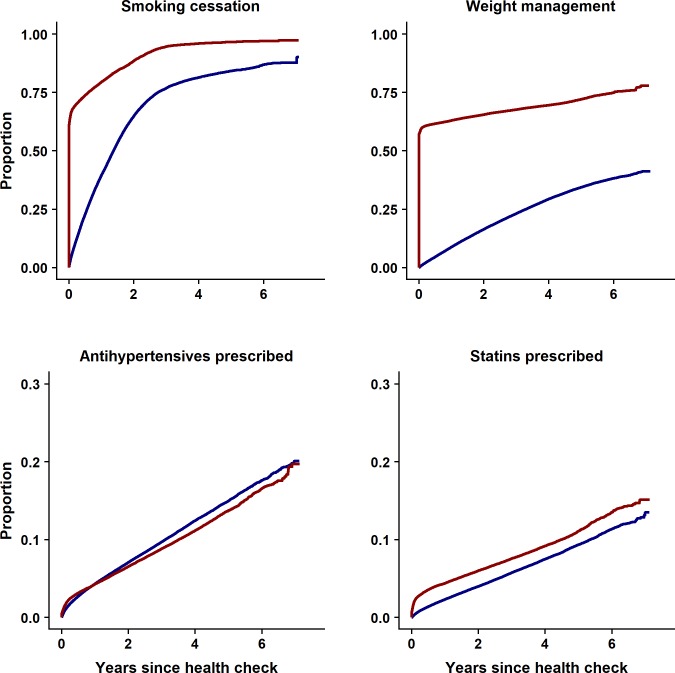
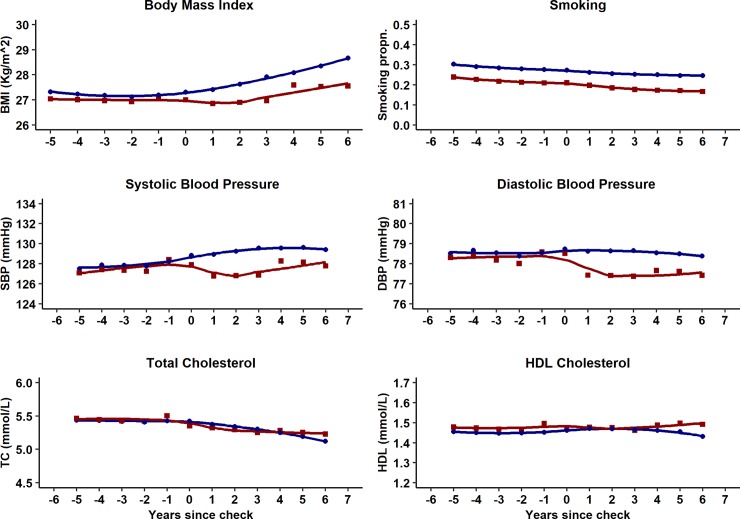
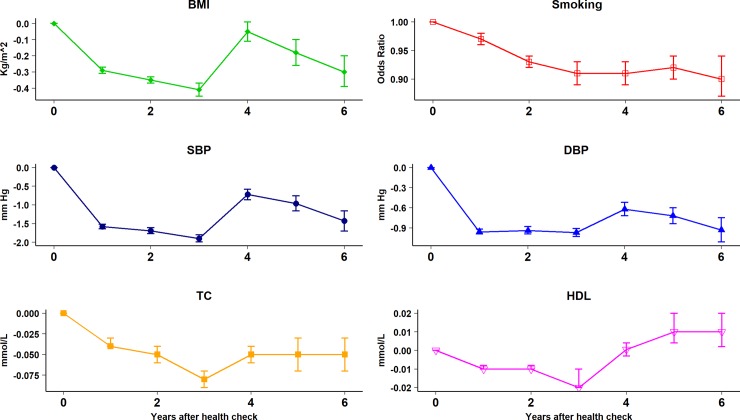
Methods and findings: A controlled interrupted time series study was conducted. Participants were registered with general practices in the Clinical Practice Research Datalink (CPRD) in England and received health checks between 1 April 2010 and 31 December 2013. Control participants, who did not receive a health check, were matched for age, sex, and general practice. Outcomes were blood pressure, body mass index (BMI), smoking, and total cholesterol (TC) and high-density lipoprotein cholesterol (HDL). Analyses estimated the net effect of health check by year, allowing for the underlying trend in risk factor values and baseline differences between cases and controls, adjusting for age, sex, deprivation, and clustering by general practice. There were 127,891 health check participants and 322,910 matched controls. Compared with controls, health check participants had lower BMI (cases mean 27.0, SD 4.8; controls 27.3, SD 5.6, Kg/m2), systolic blood pressure (SBP) (cases 129.0, SD 14.3; controls 129.3, SD 15.0, mm Hg), and smoking (21% in health check participants versus 27% in controls), but total and HDL cholesterol were similar. Health check participants were more likely to receive weight management advice (adjusted hazard ratio [HR] 5.03, 4.98 to 5.08, P < 0.001), smoking cessation interventions (HR 3.20, 3.13 to 3.27, P < 0.001), or statins (HR 1.24, 1.21 to 1.27, P < 0.001). There were net reductions in risk factor values up to six years after the check for BMI (-0.30, -0.39 to -0.20 Kg/m2, P < 0.001), SBP (-1.43, -1.70 to -1.16 mm Hg, P < 0.001), and smoking (17% in health check participants versus 25% in controls; odds ratio 0.90, 0.87 to 0.94, P < 0.001). The main study limitation was that residual confounding may be present because randomisation was not employed; health check-associated measurement introduced differential recording that might cause bias.
Conclusions: Our results suggest that people who take up a health check generally have lower risk factor values than controls and are more likely to receive risk factor interventions. Risk factor values show net reductions up to six years following a health check in BMI, blood pressure, and smoking, which may be of public health importance.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- BHF. Heart Statistics 2017. Available from: https://www.bhf.org.uk/research/heart-statistics. Cited 02 February 2018.
-
- CDC. Heart Disease Facts 2017. Available from: https://www.cdc.gov/heartdisease/facts.htm. Cited 02 February 2018.
-
- WHO. Global Heath Risks: Mortality and burden of disease attributable to selected major risks 2009. Available from: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_re.... Cited 26 January 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
