

Low dose Epigallocatechin Gallate Alleviates Experimental Colitis by Subduing Inflammatory Cells and Cytokines, and Improving Intestinal Permeability
- PMID: 31362373
- PMCID: PMC6724056
- DOI: 10.3390/nu11081743
Low dose Epigallocatechin Gallate Alleviates Experimental Colitis by Subduing Inflammatory Cells and Cytokines, and Improving Intestinal Permeability
Abstract
Background: In this study, we investigate the impact of epigallocatechin gallate (EGCG), the most abundant and potent catechin in green tea, on a mouse model of inflammatory bowel disease (IBD) and the underlying mechanisms of action.
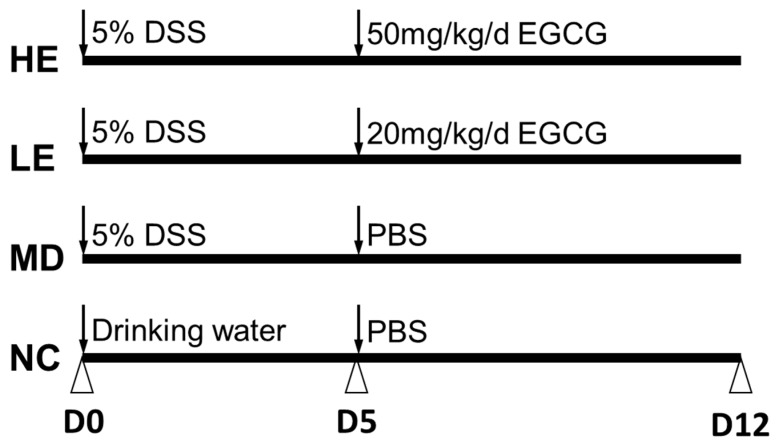
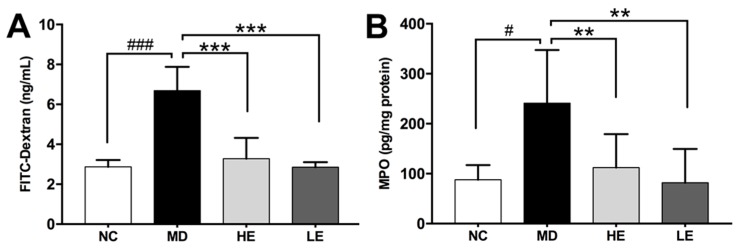
Methods: C57BL/6J mice were subjected to dextran sulfate sodium (DSS)-induced IBD-like disease and then randomly divided into three groups: Model group (MD), low-dose EGCG group (LE, 20 mg/kg/d), and high-dose EGCG group (HE, 50 mg/kg/d). DSS-induced clinical and macroscopic changes were monitored daily. Intestinal permeability was assessed by FITC-Dextran assay.
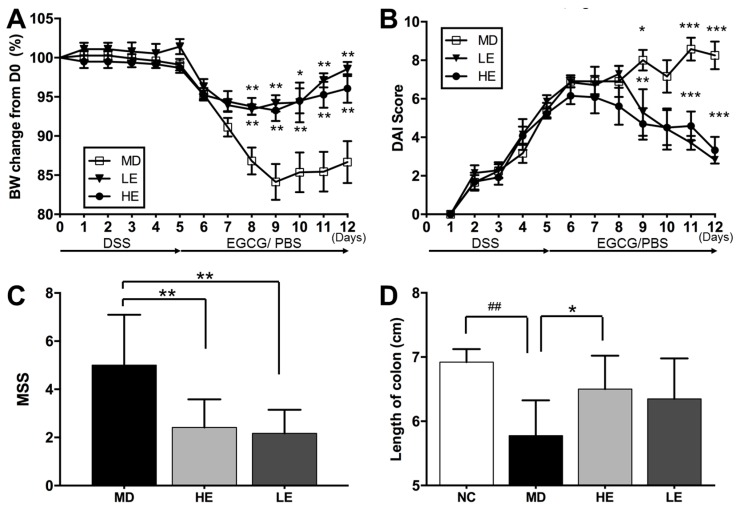
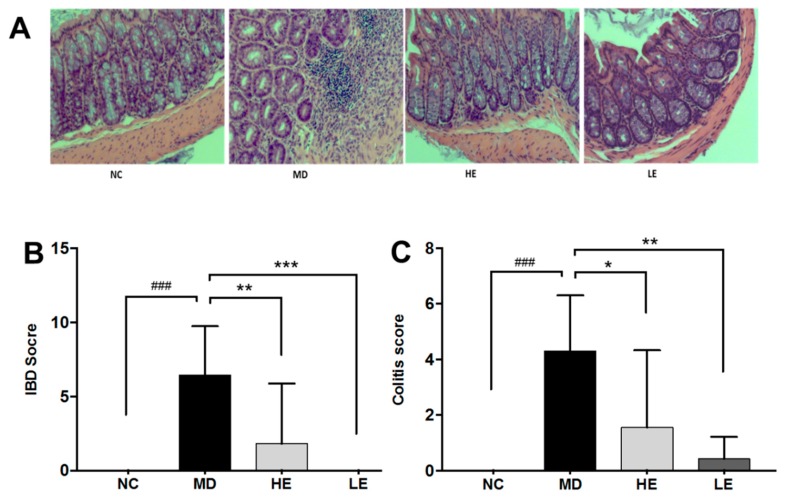
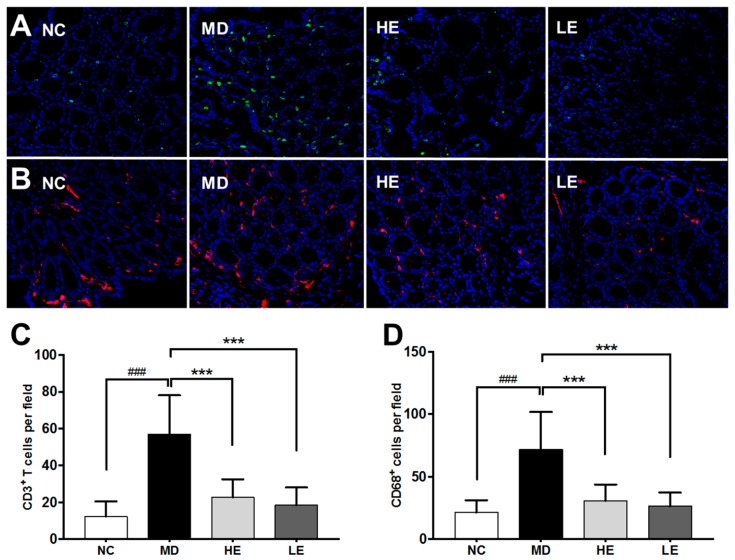
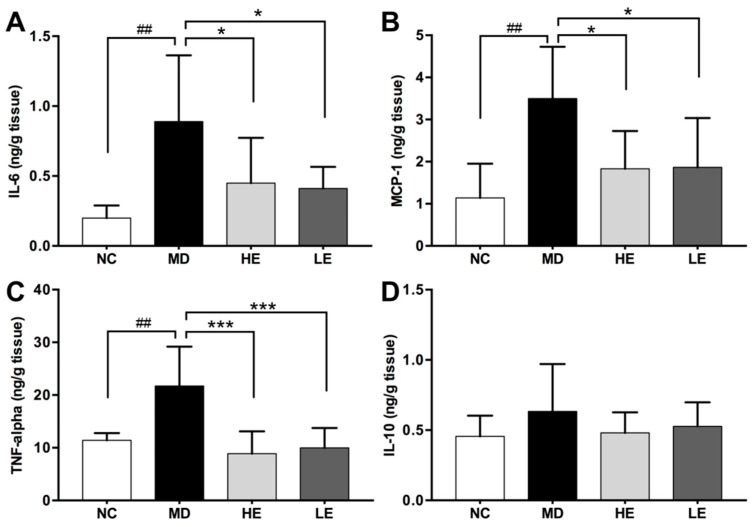
Results: Both high- and low-dose EGCG treatment alleviated clinical manifestations including body weight loss and disease activity index (DAI) of DSS-induced colitis. The DAI score was significantly improved after two days of EGCG treatment. At the end of the study, the macroscopic severity score (MSS) of HE and LE treatment groups were 2.4 ± 1.2, and 2.2 ± 1.0, respectively, significantly lower than that of the controls (5.0 ± 2.1). EGCG treatment also prevented colon shortening, and improved intestinal permeability and histopathological changes. In addition, EGCG treatment attenuated colon inflammation by suppressing colonic levels of pro-inflammatory cytokines IL-6, MCP-1, and TNF-alpha, and inhibited CD3+ T cell and CD68+ macrophage infiltration.
Conclusion: EGCG is effective in inflammatory colitis because it reduces cellular and molecular inflammation, and reduces intestinal permeability.
Keywords: animal model; epigallocatechin gallate (EGCG), cytokines; inflammatory bowel disease.
Conflict of interest statement
We have no conflict of interest to declare.
Figures
References
-
- Molodecky N.A., Soon I.S., Rabi D.M., Ghali W.A., Ferris M., Chernoff G., Benchimol E.I., Panaccione R., Ghosh S., Barkema H.W., et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54. doi: 10.1053/j.gastro.2011.10.001. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
