

Subclinical Atherosclerosis Imaging in People Living with HIV
- PMID: 31362391
- PMCID: PMC6723163
- DOI: 10.3390/jcm8081125
Subclinical Atherosclerosis Imaging in People Living with HIV
Abstract
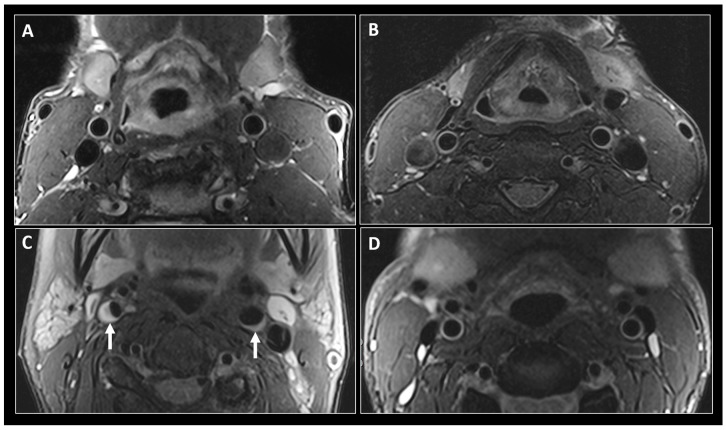
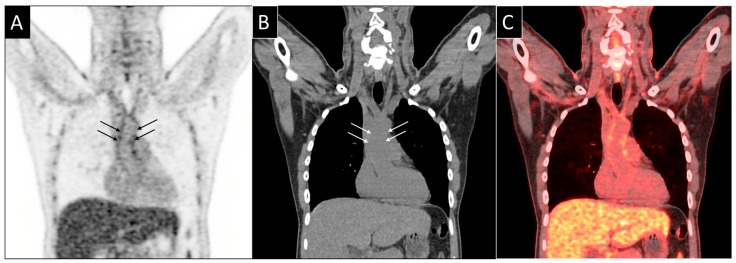
In many, but not all studies, people living with HIV (PLWH) have an increased risk of coronary artery disease (CAD) events compared to the general population. This has generated considerable interest in the early, non-invasive detection of asymptomatic (subclinical) atherosclerosis in PLWH. Ultrasound studies assessing carotid artery intima-media thickness (CIMT) have tended to show a somewhat greater thickness in HIV+ compared to HIV-, likely due to an increased prevalence of cardiovascular (CV) risk factors in PLWH. Coronary artery calcification (CAC) determination by non-contrast computed tomography (CT) seems promising to predict CV events but is limited to the detection of calcified plaque. Coronary CT angiography (CCTA) detects calcified and non-calcified plaque and predicts CAD better than either CAC or CIMT. A normal CCTA predicts survival free of CV events over a very long time-span. Research imaging techniques, including black-blood magnetic resonance imaging of the vessel wall and 18F-fluorodeoxyglucose positron emission tomography for the assessment of arterial inflammation have provided insights into the prevalence of HIV-vasculopathy and associated risk factors, but their clinical applicability remains limited. Therefore, CCTA currently appears as the most promising cardiac imaging modality in PLWH for the evaluation of suspected CAD, particularly in patients <50 years, in whom most atherosclerotic coronary lesions are non-calcified.
Keywords: HIV infection; accelerated atherosclerosis; carotid intima-media thickness; coronary CT angiography; coronary calcium scoring; fluorodeoxyglucose positron emission tomography; magnetic resonance angiography; subclinical coronary artery disease.
Conflict of interest statement
P.E.T.’s institution has received research grants and advisory fees from ViiV and Gilead. The research of I.C.S., R.R.B., H.K., and P.E.T. supported by the Swiss National Science Foundation and the Swiss HIV Cohort Study. The other authors declare no conflicts of interest.
Figures
Similar articles
-
Relationship between carotid atherosclerosis and coronary artery calcification in asymptomatic diabetic patients: A prospective multicenter study.Clin Cardiol. 2017 Sep;40(9):752-758. doi: 10.1002/clc.22727. Epub 2017 May 25. Clin Cardiol. 2017. PMID: 28543093 Free PMC article.
-
Prevalence and Characterization of Subclinical Coronary Atherosclerotic Plaque with CT among Individuals with HIV: Results from the Canadian HIV and Aging Cohort Study.Radiology. 2021 Jun;299(3):571-580. doi: 10.1148/radiol.2021203297. Epub 2021 Apr 20. Radiology. 2021. PMID: 33876969
-
Early atherosclerosis detection in asymptomatic patients: a comparison of carotid ultrasound, coronary artery calcium score, and coronary computed tomography angiography.Can J Cardiol. 2013 Dec;29(12):1687-94. doi: 10.1016/j.cjca.2013.10.003. Epub 2013 Oct 5. Can J Cardiol. 2013. PMID: 24267808
-
Coronary Artery Microcalcification: Imaging and Clinical Implications.Diagnostics (Basel). 2019 Sep 23;9(4):125. doi: 10.3390/diagnostics9040125. Diagnostics (Basel). 2019. PMID: 31547506 Free PMC article. Review.
-
Is carotid intima-media thickness as predictive as other noninvasive techniques for the detection of coronary artery disease?Arterioscler Thromb Vasc Biol. 2014 Jul;34(7):1341-5. doi: 10.1161/ATVBAHA.113.302075. Epub 2014 Apr 24. Arterioscler Thromb Vasc Biol. 2014. PMID: 24764454 Review.
Cited by
-
A Comprehensive Review of the Manifestation of Cardiovascular Diseases in HIV Patients.Cureus. 2025 Jan 15;17(1):e77509. doi: 10.7759/cureus.77509. eCollection 2025 Jan. Cureus. 2025. PMID: 39958097 Free PMC article. Review.
-
Immune Dysregulation in Ischemic Heart Disease Among Individuals with Human Immunodeficiency Virus.Heart Fail Clin. 2025 Apr;21(2):227-239. doi: 10.1016/j.hfc.2024.12.005. Epub 2025 Jan 30. Heart Fail Clin. 2025. PMID: 40107801 Review.
-
Cardiovascular risk assessment in inflammatory bowel disease with coronary calcium score.Ann Med Surg (Lond). 2024 Jan 4;86(3):1496-1505. doi: 10.1097/MS9.0000000000001652. eCollection 2024 Mar. Ann Med Surg (Lond). 2024. PMID: 38463108 Free PMC article. Review.
-
[68Ga]Ga-Pentixafor for PET Imaging of Vascular Expression of CXCR-4 as a Marker of Arterial Inflammation in HIV-Infected Patients: A Comparison with 18F[FDG] PET Imaging.Biomolecules. 2020 Dec 3;10(12):1629. doi: 10.3390/biom10121629. Biomolecules. 2020. PMID: 33287237 Free PMC article.
-
Role of Brain Arterial Remodeling in HIV-Associated Cerebrovascular Outcomes.Front Neurol. 2021 Jun 22;12:593605. doi: 10.3389/fneur.2021.593605. eCollection 2021. Front Neurol. 2021. PMID: 34239489 Free PMC article. Review.
References
-
- Mozaffarian D., Benjamin E.J., Go A.S., Arnett D.K., Blaha M.J., Cushman M., Das S.R., de Ferranti S., Després J., Fullerton H.J., et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2015;133:38–360. doi: 10.1161/CIR.0000000000000350. - DOI - PubMed
-
- Shah A.S.V., Stelzle D., Lee K.K., Beck E.J., Alam S., Clifford S., Longenecker C.T., Strachan F., Bagchi S., Whiteley W., et al. Global Burden of Atherosclerotic Cardiovascular Disease in People Living With HIV. Circulation. 2018;138:1100–1112. doi: 10.1161/CIRCULATIONAHA.117.033369. - DOI - PMC - PubMed
-
- Weber R., Ruppik M., Rickenbach M., Spoerri A., Furrer H., Battegay M., Cavassini M., Calmy A., Bernasconi E., Schmid P., et al. Decreasing mortality and changing patterns of causes of death in the Swiss HIV Cohort Study. HIV Med. 2013;14:195–207. doi: 10.1111/j.1468-1293.2012.01051.x. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
