

Pathological severity determines the renal recovery for anti-myeloperoxidase antibody-associated vasculitis requiring dialysis at disease onset: a retrospective study
- PMID: 31362703
- PMCID: PMC6668067
- DOI: 10.1186/s12882-019-1487-7
Pathological severity determines the renal recovery for anti-myeloperoxidase antibody-associated vasculitis requiring dialysis at disease onset: a retrospective study
Abstract
Background: Many patients with anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) need dialysis at disease onset due to severe kidney injury. Determining whether they can become dialysis independent is an important clinical assessment.
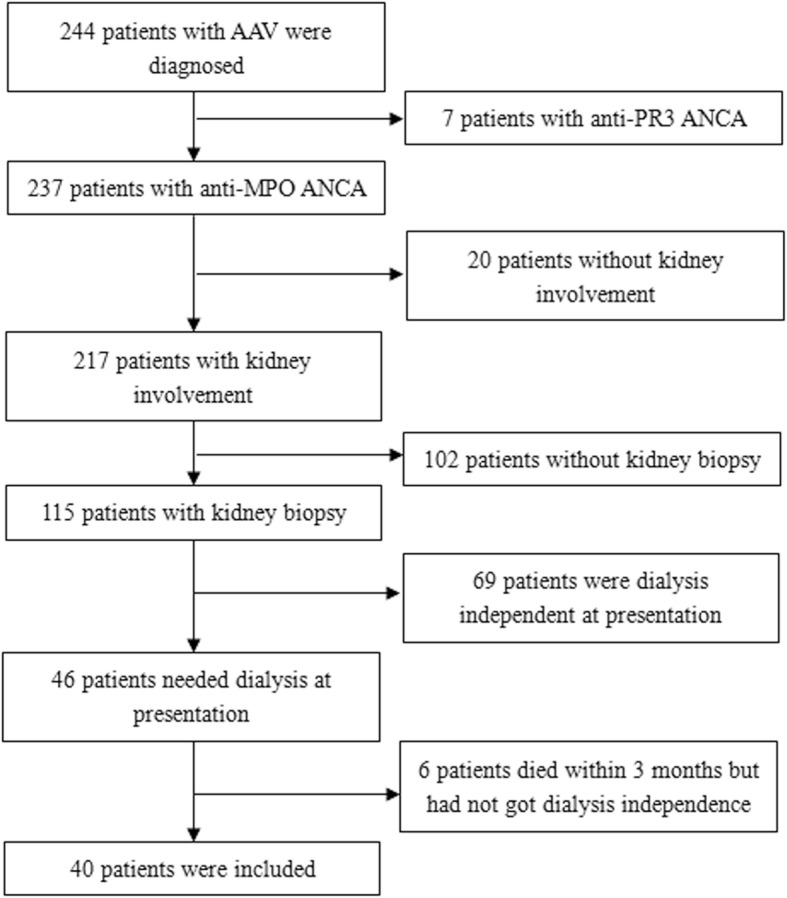
Methods: Forty kidney biopsy-proved myeloperoxidase (MPO)-ANCA associated AAV patients who required dialysis at disease onset were enrolled. Relationships between laboratory and pathological characteristics and prognoses were analyzed.
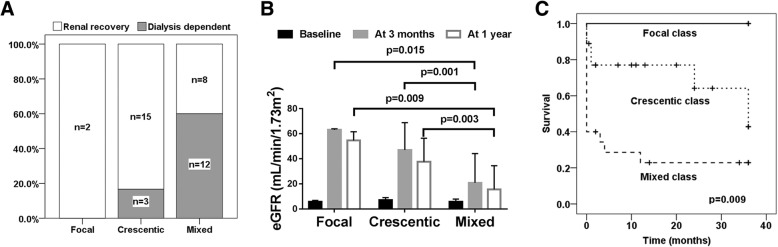
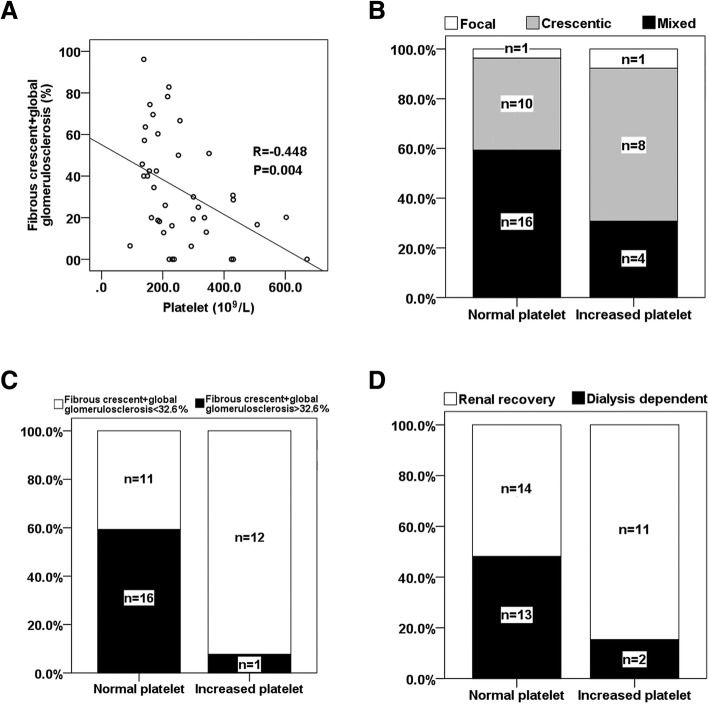
Results: Twenty-five patients obtained dialysis independence within 3 months, while the other 15 patients remained dialysis dependent. No sclerotic class was identified among the 40 patients. Only two biopsies exhibited focal class diagnoses and both these patients recovered their renal function. The renal recovery rate of the 20 patients with mixed class was significantly lower than that of the 18 patients with crescentic class (40.0% vs. 83.3%, p = 0.006). Receiver operating characteristics (ROC) curves showed fibrous crescent+global glomerulosclerosis greater than 32.6% was a strong predictor of dialysis dependence with a sensitivity of 93.3% and specificity of 88.0%. When the percentage of fibrous crescent+global glomerulosclerosis exceeded 47.9%, dialysis independence was not possible. Correlation analysis indicated that platelet counts were negatively correlated with the percentage of fibrous crescent+global glomerulosclerosis (R = -0.448, p = 0.004). Most patients with increased platelets (84.62%) obtained renal recovery. Compared with methylprednisolone pulse therapy, plasma exchange accelerated renal recovery (29.4 ± 15.6 vs. 41.4 ± 11.7 days, p = 0.039).
Conclusions: For MPO-ANCA AAV who required dialysis at disease onset, crescentic and mixed classes accounted for the majority of patients in our cohort. The renal outcome of mixed class patients was worse than that of crescentic class. A high proportion of fibrous crescent+global glomerulosclerosis is a predictor of dialysis dependence. Increased platelet count is associated with active and reversible renal lesions.
Keywords: Antineutrophil cytoplasmic antibody; Dialysis; Histopathologic classification; Myeloperoxidase; Renal biopsy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
High anti-neutrophil cytoplasmic antibody titers are associated with the requirement of permanent dialysis in patients with myeloperoxidase-ANCA-associated vasculitis.J Formos Med Assoc. 2019 Oct;118(10):1408-1415. doi: 10.1016/j.jfma.2019.05.004. Epub 2019 May 24. J Formos Med Assoc. 2019. PMID: 31133523
-
ANCA positive crescentic glomerulonephritis outcome in a Central East European cohort: a retrospective study.BMC Nephrol. 2015 Jun 30;16:90. doi: 10.1186/s12882-015-0091-8. BMC Nephrol. 2015. PMID: 26123651 Free PMC article.
-
Outcome Predictors of Biopsy-Proven Myeloperoxidase-Anti-Neutrophil Cytoplasmic Antibody-Associated Glomerulonephritis.Front Immunol. 2021 Feb 4;11:607261. doi: 10.3389/fimmu.2020.607261. eCollection 2020. Front Immunol. 2021. PMID: 33613528 Free PMC article.
-
Risk Factors for Renal Survival in Chinese Patients with Myeloperoxidase-ANCA-Associated GN.Clin J Am Soc Nephrol. 2017 Mar 7;12(3):417-425. doi: 10.2215/CJN.06200616. Epub 2017 Feb 1. Clin J Am Soc Nephrol. 2017. PMID: 28148558 Free PMC article.
-
ANCA-associated vasculitis with renal involvement.J Nephrol. 2018 Apr;31(2):197-208. doi: 10.1007/s40620-017-0412-z. Epub 2017 May 30. J Nephrol. 2018. PMID: 28560688 Review.
Cited by
-
Histopathological Findings Predict Renal Recovery in Severe ANCA-Associated Vasculitis Requiring Intensive Care Treatment.Front Med (Lausanne). 2021 Feb 9;7:622028. doi: 10.3389/fmed.2020.622028. eCollection 2020. Front Med (Lausanne). 2021. PMID: 33634143 Free PMC article.
-
Development of a Kidney Prognostic Score in a Japanese Cohort of Patients With Antineutrophil Cytoplasmic Autoantibody Vasculitis.Kidney Int Rep. 2024 Jan 8;9(3):611-623. doi: 10.1016/j.ekir.2024.01.007. eCollection 2024 Mar. Kidney Int Rep. 2024. PMID: 38481514 Free PMC article.
-
Prognostic Value of Neutrophil-To-Lymphocyte Ratio and Platelet-To-Lymphocyte Ratio for Renal Outcomes in Patients with Rapidly Progressive Glomerulonephritis.J Clin Med. 2020 Apr 15;9(4):1128. doi: 10.3390/jcm9041128. J Clin Med. 2020. PMID: 32326552 Free PMC article.
-
Clinicopathological characteristics and outcomes of anti-neutrophil cytoplasmic autoantibody-related renal vasculitis with hyperuricemia: a retrospective case-control study.Sci Rep. 2021 Jan 21;11(1):2002. doi: 10.1038/s41598-021-81664-z. Sci Rep. 2021. PMID: 33479426 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
